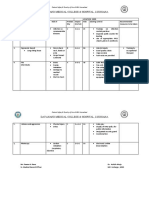
Deficiency of Case Sheet
Deficiency of Case Sheet
Download as pptx, pdf, or txt
You might also like
- Audit Checklist For HICDocument3 pagesAudit Checklist For HICbalbirchildrenNo ratings yet
- Er Triage PolicyDocument10 pagesEr Triage PolicyAl Rahim Medical OnlineNo ratings yet
- Mortuary Services Checklist - Random 202335531Document4 pagesMortuary Services Checklist - Random 202335531Marion KonesNo ratings yet
- Procedure(s) Guide Collection, Identification, Handling, Safe Transportation, Processing andDocument3 pagesProcedure(s) Guide Collection, Identification, Handling, Safe Transportation, Processing andVEEKU HOSPITALSNo ratings yet
- Project Welike 1st Year PresentationDocument44 pagesProject Welike 1st Year Presentationshourav upadhay100% (1)
- Incident Reporting Form PDFDocument2 pagesIncident Reporting Form PDFdeeptiNo ratings yet
- Cop 2 Emergency Department ManualDocument34 pagesCop 2 Emergency Department Manualanitha100% (1)
- 15 Define Process To Whom The Patient Record Can Be ReleasedDocument8 pages15 Define Process To Whom The Patient Record Can Be ReleasedSanjay KadamNo ratings yet
- 2 Process Addresses Discharge of All Patients Including Medico-Legal Cases and Patients Leaving Against Medical Advice.Document6 pages2 Process Addresses Discharge of All Patients Including Medico-Legal Cases and Patients Leaving Against Medical Advice.Sanjay Kadam100% (1)
- HIRA MRD FinalDocument4 pagesHIRA MRD FinalSwati joshiNo ratings yet
- Effective CommunicationDocument11 pagesEffective CommunicationEsamNo ratings yet
- Pre - de - Coding NabhDocument43 pagesPre - de - Coding NabhDr Ananta Kumari ChaurasiaNo ratings yet
- Blackrock Inc: Public NyseDocument4 pagesBlackrock Inc: Public NyseabhijaisNo ratings yet
- MRD Guidline NABHDocument3 pagesMRD Guidline NABHharpreet kaur brar100% (1)
- Hope RequirementsDocument7 pagesHope Requirementscorona virusNo ratings yet
- AAC.6 FinalDocument5 pagesAAC.6 FinalJatoveda HaldarNo ratings yet
- FMS Round RegisterDocument6 pagesFMS Round RegistertanishaNo ratings yet
- 5thEdGuidelines Converted1Document226 pages5thEdGuidelines Converted1ravi4ramaniNo ratings yet
- 03 Mom RDocument18 pages03 Mom RselvarajNo ratings yet
- Prescription Audit FormDocument6 pagesPrescription Audit FormZothankhuma100% (1)
- New MRD Manual 12-1-15Document12 pagesNew MRD Manual 12-1-15aarti Hinge100% (1)
- PRESENTATION 1. Grieviance Redressal CommitteeDocument25 pagesPRESENTATION 1. Grieviance Redressal CommitteeBAHHEP BAHHEPNo ratings yet
- Medical Adt CHK LST Surgical CasesDocument2 pagesMedical Adt CHK LST Surgical CasesmedicodikshakaushalNo ratings yet
- Active File Audit For HospitalDocument4 pagesActive File Audit For HospitalRahul IndalkarNo ratings yet
- Final Admission PolicyDocument6 pagesFinal Admission Policytanisha100% (1)
- MRI Safety Screening Form - Amended - 30NOV2016Document1 pageMRI Safety Screening Form - Amended - 30NOV2016FC LOONNo ratings yet
- NABH Pre Accreditation Entry LevelDocument12 pagesNABH Pre Accreditation Entry LevelAmit TyagiNo ratings yet
- IPD Feedbac FormDocument3 pagesIPD Feedbac FormHiral PanchalNo ratings yet
- Document Name Document Number Date Created Date Implemented Name: Designation: Signature: Name: Designation: SignatureDocument49 pagesDocument Name Document Number Date Created Date Implemented Name: Designation: Signature: Name: Designation: Signaturecorona virusNo ratings yet
- Quality Improvement Project - AidetDocument7 pagesQuality Improvement Project - AidetAnirban RoyNo ratings yet
- PROSPECT APACHE II Calculation WorksheetDocument1 pagePROSPECT APACHE II Calculation WorksheetHamza MahmoudNo ratings yet
- Nabh ChecklistDocument2 pagesNabh ChecklistJatoveda Haldar100% (1)
- MRD Report FormatDocument2 pagesMRD Report FormatKeshava NagalkarNo ratings yet
- Report On HIRA in Fortis Hospital AmritsarDocument15 pagesReport On HIRA in Fortis Hospital AmritsarUmar LoneNo ratings yet
- Code Red DrillDocument1 pageCode Red DrillPayal ThakkerNo ratings yet
- Competency Assessment For Infection Control NurseDocument2 pagesCompetency Assessment For Infection Control Nursenseducation.mahgNo ratings yet
- IC Clinical Risk Register 9419Document3 pagesIC Clinical Risk Register 9419Sathappan KasiNo ratings yet
- NABH 5th Edition - COP - Emergency ServicesDocument14 pagesNABH 5th Edition - COP - Emergency ServicesanithaNo ratings yet
- NC DetailsDocument3 pagesNC DetailsAHA IKDRC-ITSNo ratings yet
- Medication Chart With Error Prone Abbreviation1Document1 pageMedication Chart With Error Prone Abbreviation1Nidhi VijanNo ratings yet
- Signage and Display in HospitalsDocument18 pagesSignage and Display in HospitalsDivaKant MisraNo ratings yet
- 63 MdroDocument3 pages63 MdroerwindaNo ratings yet
- IPSG May28Document62 pagesIPSG May28S. Pichammal - Quality ManagerNo ratings yet
- COP 3 & PFR 1.5 - Care of Vulnerable PatientsDocument4 pagesCOP 3 & PFR 1.5 - Care of Vulnerable Patientsn_robinNo ratings yet
- Surgical Quality Assurance ProgramDocument7 pagesSurgical Quality Assurance Programilyaskhosa032No ratings yet
- Emergency Admission & Transfer RegisterDocument21 pagesEmergency Admission & Transfer RegisterAnkur Singh0% (1)
- List of Hospital Committees and Teams For NABH Accreditation PreparationDocument6 pagesList of Hospital Committees and Teams For NABH Accreditation PreparationSanjay Kadam100% (1)
- 6 Opening Presentation - NABH-2020Document29 pages6 Opening Presentation - NABH-2020priya100% (1)
- Adityavardhan Hospital: Policies & ProceduresDocument4 pagesAdityavardhan Hospital: Policies & ProceduresSanjay KadamNo ratings yet
- Gap Report Astha HospitalDocument49 pagesGap Report Astha HospitalNidhi Vijan100% (1)
- Prescription Audit of Cardiac Drugs in CardiacDocument15 pagesPrescription Audit of Cardiac Drugs in CardiacInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 11 End of Life CareDocument5 pages11 End of Life CareSree KumarNo ratings yet
- Management of MedicationDocument32 pagesManagement of Medicationsanjay100% (1)
- Nabh Work PlanDocument4 pagesNabh Work Planuraza.octavo0% (1)
- Nabh Entry Level StandardsDocument46 pagesNabh Entry Level StandardsDr. Suhas SodalNo ratings yet
- Medical Audit Checklist Active File AuditDocument2 pagesMedical Audit Checklist Active File AuditCOO TOP STARNo ratings yet
- Nmhaacqsp7 Quality Assurance Programme For ImagingDocument9 pagesNmhaacqsp7 Quality Assurance Programme For ImagingAniruddha ChatterjeeNo ratings yet
- AuditDocument3 pagesAuditMr. BamsNo ratings yet
- Nabh PolicyDocument4 pagesNabh PolicySanjay KadamNo ratings yet
- NABH 5th and 6th Edition ChangesDocument8 pagesNABH 5th and 6th Edition Changesaas100% (1)
- Standards For MIS - 2nd Edition - EditedDocument72 pagesStandards For MIS - 2nd Edition - Editedrohitnt93_979373629No ratings yet
- Form 12BBDocument1 pageForm 12BBGopala KrishnanNo ratings yet
- Letter Re APA Breach 10.31.23Document2 pagesLetter Re APA Breach 10.31.23Mitchell BlackNo ratings yet
- South Asian Association For Regional Cooperation (Saarc)Document4 pagesSouth Asian Association For Regional Cooperation (Saarc)Saba PervezNo ratings yet
- Chennai WUDC Adjudicator BriefingDocument12 pagesChennai WUDC Adjudicator BriefingAaron VillaflorNo ratings yet
- CLD - Bao3404 Tutorial GuideDocument7 pagesCLD - Bao3404 Tutorial GuideShi MingNo ratings yet
- Mumbai To AurangabadDocument1 pageMumbai To AurangabadShailesh KumarNo ratings yet
- Dar-E-Arqam Girls College Sargodha Test No 1 (CH 1) : Q#1 Mcqs A B C DDocument8 pagesDar-E-Arqam Girls College Sargodha Test No 1 (CH 1) : Q#1 Mcqs A B C DsabaNo ratings yet
- Cash BudgetsDocument23 pagesCash Budgetsarjun sachdevNo ratings yet
- United States v. Jose Rafael Abello-Silva, 948 F.2d 1168, 10th Cir. (1991)Document21 pagesUnited States v. Jose Rafael Abello-Silva, 948 F.2d 1168, 10th Cir. (1991)Scribd Government DocsNo ratings yet
- Complaint COMES NOW, The Petitioner Together With The Undersigned Counsel To This Honorable CourtDocument2 pagesComplaint COMES NOW, The Petitioner Together With The Undersigned Counsel To This Honorable CourtPaul Claro CágroNo ratings yet
- (1.) Horizontal or Trend Analysis Balance Sheet Comparative Balance SheetDocument6 pages(1.) Horizontal or Trend Analysis Balance Sheet Comparative Balance Sheetmariolan_amigoNo ratings yet
- Avaya Control Manager Overview and Specification: Release 9.0 Issue 2 July 2020Document109 pagesAvaya Control Manager Overview and Specification: Release 9.0 Issue 2 July 2020Chau TranNo ratings yet
- 4 - Complaint & Reply LetterDocument38 pages4 - Complaint & Reply LetterDanial AfiqNo ratings yet
- Webank Leading Digital BankDocument7 pagesWebank Leading Digital BankrobynxjNo ratings yet
- City of Cotabato Affidavit of Complaint Ivana Y. MaylawitDocument6 pagesCity of Cotabato Affidavit of Complaint Ivana Y. MaylawitAlianna Arnica MambataoNo ratings yet
- AVFTB QuotesDocument12 pagesAVFTB QuotesMeshal SattarNo ratings yet
- 4 SalariesDocument6 pages4 SalariesSrinishaNo ratings yet
- Review Questions in ElemagDocument17 pagesReview Questions in ElemagHarold AntonioNo ratings yet
- Promoters and Pre-Incoporation NotesDocument11 pagesPromoters and Pre-Incoporation NotesAgitha GunasagranNo ratings yet
- Harshad Mehta ScamDocument22 pagesHarshad Mehta Scamshashwat tripathiNo ratings yet
- Del Rosario v. Del Rosario and CADocument9 pagesDel Rosario v. Del Rosario and CAVeniceAbuzmanBrualNo ratings yet
- Complete Goldfranks Toxicologic Emergencies 10 PDF For All ChaptersDocument10 pagesComplete Goldfranks Toxicologic Emergencies 10 PDF For All Chaptersauxanebezzi100% (7)
- Basic OT NotesDocument20 pagesBasic OT NotesNimshiNo ratings yet
- 2006 Daihatsu Terios Engine Service ManualDocument1 page2006 Daihatsu Terios Engine Service ManualLuis Antonio Castillo Arispe57% (7)
- Resume - Hiba LarrachDocument1 pageResume - Hiba Larrachhi-bNo ratings yet
- Asia Prod vs. Lolita LeeDocument6 pagesAsia Prod vs. Lolita LeeTats YumulNo ratings yet
- CAF 2 TAX Autumn 2020Document6 pagesCAF 2 TAX Autumn 2020duocarecoNo ratings yet
- HA System Software Installation Guide (Solaris) - (V100R002C01 - 06)Document289 pagesHA System Software Installation Guide (Solaris) - (V100R002C01 - 06)Adrian FlorensaNo ratings yet