Acceptance and Commitment Therapy For Children
Acceptance and Commitment Therapy For Children
Uploaded by
ClaudiaCopyright:
Available Formats
Acceptance and Commitment Therapy For Children
Acceptance and Commitment Therapy For Children
Uploaded by
ClaudiaOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Copyright:
Available Formats
Acceptance and Commitment Therapy For Children
Acceptance and Commitment Therapy For Children
Uploaded by
ClaudiaCopyright:
Available Formats
Author's Accepted Manuscript
Acceptance and commitment therapy for
children: A systematic review of intervention
studies
Jessica Swain, Karen Hancock, Angela Dixon,
Jenny Bowman
www.elsevier.com/locate/jcbs
PII: S2212-1447(15)00004-6
DOI: http://dx.doi.org/10.1016/j.jcbs.2015.02.001
Reference: JCBS80
To appear in: Journal of Contextual Behavioral Science
Received date: 31 March 2014
Revised date: 20 December 2014
Accepted date: 11 February 2015
Cite this article as: Jessica Swain, Karen Hancock, Angela Dixon, Jenny
Bowman, Acceptance and commitment therapy for children: A systematic
review of intervention studies, Journal of Contextual Behavioral Science, http://dx.
doi.org/10.1016/j.jcbs.2015.02.001
This is a PDF file of an unedited manuscript that has been accepted for
publication. As a service to our customers we are providing this early version of
the manuscript. The manuscript will undergo copyediting, typesetting, and
review of the resulting galley proof before it is published in its final citable form.
Please note that during the production process errors may be discovered which
could affect the content, and all legal disclaimers that apply to the journal
pertain.
Title: Acceptance and Commitment Therapy for children: A systematic review of intervention
studies
Author names/affiliations: Jessica Swain a, b, Karen Hancock a, b, Angela Dixon a, Jenny
Bowman b
a
Department of Psychological Medicine, The Children’s Hospital at Westmead, Sydney NSW
2145
b
School of Psychology, The University of Newcastle, Newcastle NSW 2308
Corresponding author: Jessica Swain; Ph: +61 410 452 140; E: [email protected]
Current postal address: Jessica Swain Mental Health & Psychology Section, Lavarack Health
Centre, Lavarack Barracks, Townsville QLD Australia 4813
Introduction
Acceptance and Commitment Therapy (ACT) is a contemporary behavioural and cognitive
therapy that works to foster increasing flexibility in response to thoughts, feelings and sensations
through processes of mindfulness, acceptance, and behaviour change (S. C. Hayes, Levin,
Plumb-Vilardaga, Villatte, & Pistorello, 2013; Wilson, Bordieri, Flynn, Lucas, & Slater, 2011).
In ACT the focus of change interventions is the context in which psychological phenomena
occur, rather than the direct change attempts of their content/validity or frequency, as typified by
traditional cognitive behaviour therapy (CBT; Blackledge, Ciarrochi, & Deane, 2009; S. C.
Hayes, 2004; S. C. Hayes, Villatte, Levin, & Hildebrandt, 2011).
ACT is underpinned by a theoretical framework, termed relational frame theory (RFT; S. C.
Hayes et al., 2011). RFT focuses on human language and cognitive processes and suggests that
with language development we learn to continually derive relations between events. From
childhood we learn to relate events to each other on the basis of social convention and to derive
meaning from events on the basis of this relating, termed in ACT “learned derivation” (Luoma,
Hayes, & Walser, 2007). For example, during early language training interactions, children are
often shown objects and asked to repeat their names. A mother may then clap her hands, or say,
“That’s right, a car!”, reinforcing the spoken word “car” with the object, car. The child may also
be taught the name of the car, so object-word and word-object relation is explicitly trained. With
sufficient repetitions learned derivation occurs. The child is then able to generalise the spoken
word car to a toy car, and to the printed words “toy car”, and vice-versa.
Whilst learned derivation offers evolutionary advantages, it can also act as a hindrance. When
language is taken literally this can result in a “fusion” with thinking (i.e. experience one’s own
thoughts and beliefs as literally true), and can lead to pain (Harris, 2009). In ACT this is termed
cognitive fusion. To illustrate, fusing with the thought that “life is unbearable” might produce
depressive symptoms despite the existence of various things required to live a full life, such as
meaningful employment and supportive relationships (S. C. Hayes, Pistorello, & Levin, 2012).
Cognitive fusion in turn leads to a whole host of reactions, known as “experiential avoidance”,
such as excessive use of problem solving, active efforts to escape or avoid feelings, and
entanglement in thinking; methods employed as a way to solve our pain (Luoma et al., 2007).
These methods result in a loss of contact with the present, belief in negative stories about
ourselves, and rigidity in our way of living. Life becomes less about opening up in the pursuit of
things that are important, but tends to result in an overall narrowing of living to support freedom
from distress (Harris, 2009). In ACT this is termed psychological inflexibility.
ACT employs six interrelational core therapeutic processes that form a “hexaflex” model of
psychological flexibility; acceptance, cognitive defusion, mindfulness, self-as-context,
committed action, and valued living (Luoma et al., 2007). Acceptance is employed as the
antithesis to experiential avoidance. The focus is on opening up to thoughts, feelings and
sensations in order to increase the behaviour repertoire and allow for action that is in line with
what is important (S. C. Hayes et al., 2012). To counteract cognitive fusion, clients learn to
change the way they relate to their thoughts, and thereby decrease their attachment to these. For
children, metaphors and experiential exercises help the child recognise a thought for what it is,
just a bunch of words, and not what it says it is. Mindfulness is utilised to reduce problematic
attentional patterns, that are past focused or future orientated (S. C. Hayes et al., 2012), in order
to reduce cognitive errors such as rumination (past) or catastrophising (future). Clients are taught
mindfulness approaches to increase their skills in staying present focused. Approaches may
range from formal meditation exercises to deliberately averting “auto-pilot” by deliberately
focusing on the here-and-now experience of activities of daily living such as breathing, walking
or riding a bike (Harris, 2009). Self-as-context is best conceptualised as a perspective taken from
the sense of self, or the ability of humans to consciously notice themselves doing, thinking or
experiencing things whilst they are occurring. Therapeutically, contact with the self-as-context is
achieved via mindfulness and perspective-taking (S. C. Hayes et al., 2012). Values identification
is employed to assist in living life the way that is meaningful to each individual, supporting the
identification of those tenets that may act as a compass to future action and as intrinsic
reinforcers to the continuation of this behaviour (S. C. Hayes et al., 2012). For children this is
working through what really matters to them at school, home and/or in their friendships for
example. Committed action advocates engaging in behaviour that is in line with personal values
for living, moment-by-moment, this often takes the appearance of behaviour change goals such
as behavioural activation or exposure (S. C. Hayes et al., 2012). These approaches from the
hexaflex are deployed to foster the attainment of increasingly flexible methods of managing
challenging cognitions, emotions or sensations, thereby diminishing their deleterious behavioural
consequences (Arch & Craske, 2008).
ACT has a growing evidence base in the treatment of adult psychopathology, with numerous
reviews and meta-analyses demonstrating its efficacy (e.g., S. C. Hayes, Luoma, Bond, Masuda,
& Lillis, 2006; Levin & Hayes, 2009; Ruiz, 2012). There has also been considerable interest in
the adaptation and assessment of the suitability of ACT approaches among child and adolescent
populations (e.g., Coyne, McHugh, & Martinez, 2011; Greco, Blackledge, Coyne, & Ehrenreich,
2005; Murrell & Scherbarth, 2006). Reviews have found other psychotherapeutic approaches,
such as traditional CBT, to be effective in the treatment of children with various presenting
problems (AACAP, 2007, 2012; James, James, Cowdrey, Soler, & Choke, 2013; Weisz,
McCarty, & Valeri, 2006). However, their effectiveness has been found to be modest (Weisz et
al., 2006) and/or superior to no treatment, but not active control conditions (James et al., 2013).
Finally, a recent review concluded that CBT is not necessarily the most effective form of
treatment for young people, but the only one that has been researched enough to provide
evidence to support its use (Creswell, Waite, & Cooper, 2014). Thus there is room for
improvement and there is a need for more rigorous research into alternative treatments to support
evidence based clinical practice.
Stemming from the cognitive behavioural tradition and with a strong theoretical basis, ACT has
been proposed as a transdiagnostic therapy, a unified treatment applicable to a range of
presenting problems and clinical diagnoses (S. C. Hayes et al., 2012; Livheim et al., 2014). One
possible mechanism through which this may occur is via ACT’s focus on experiential avoidance.
A recent review linked experiential avoidance to an array of psychopathology, finding
experiential avoidance predicts symptom severity in specific disorders, affects relapse and can
act as a mediator for psychological distress and coping (Chawla & Ostafin, 2007). If ACT were
found to work effectively as a transdiagnostic approach this would reduce the load on clinicians
to gain familiarity and competence with a whole host of diagnosis-specific evidence-based
intervention (Farchione et al., 2012). This lends itself to the potential to work across contexts,
with diverse child and adolescent populations and for clinicians to readily increase their expertise
in intervention delivery.
More research incorporating ACT processes of change is required, including into experiential
avoidance, to better elucidate this, particularly among children. Research on the ACT core
processes and their relation to QOL, or psychosocial and well-being outcomes, among children
demonstrates that these processes operate in a similar way to that of adults (for a review see
Coyne et al., 2011). Feasibility studies also offer support for the utility of mindfulness-based
approaches, such as ACT, with children (Burke, 2010). It has been argued that as children think
less literally than adults, the employment of metaphors and experiential approaches may allow
children to grasp abstract concepts through experience (O'Brien, Larson, & Murrell, 2008).
Preliminary research with children as young as four suggests provides some evidence for this
assertion (Heffner, Greco, & Eifert, 2003). Furthermore, it has been purported that children have
had less time to adopt more entrenched patterns of experiential avoidance and as such, ACT may
operate to achieve both the remediation, and prevention, of the onset of inflexible patterns of
psychological responding (Greco et al., 2005). ACT approaches may also be well-suited to
adolescents as they assist in rapport building and are less instructive (Greco et al., 2005). ACT’s
focus on experiential, or personal learning, approaches support autonomously-driven behaviour
that may be particularly appropriate for adolescents desiring increased independence who may be
non-responsive to adult direction (Hadlandsmyth, White, Nesin, & Greco, 2013). The emphasis
on values may also be pertinent for adolescents due to the exploratory nature of, and increasing
capacity for abstract thinking during, this developmental period (Greco et al., 2005).
There are two existing reviews of the ACT literature among children, however, neither have been
conducted systematically. Systematic reviews of psychotherapeutic research aim to synthesise
the academic literature, using a predefined scientific method to answer a specific clinical
question, whilst minimising bias, and support the delivery of evidence-based treatment (Mulrow,
1994). Systematic reviews also identify and analyse the methodological rigor of included studies
to support clinician’s to comprehend the validity of the findings to their clients as well as support
the conduct of future research endeavours (Mulrow, 1994). Both existing reviews of the ACT
literature for children Murrell and Scherbarth (2006) and Coyne et al. (2011) examined 15
studies, which incorporated unpublished data from conference presentations not subjected to
peer-review, parenting interventions, theoretical studies, and a study with an absence of
psychometric measures. Neither examined unpublished university theses or dissertations. Whilst
exclusive reliance on published literature in reviews may produce publication bias (McLeod &
Weisz, 2004), potentially overstating the positive nature of treatment results, it has been argued
that unpublished studies are unsuitable for systematic reviews due to their inferior
methodological rigour. However, studies that have examined the rigour of grey literature,
academic unpublished literature that has not been subjected to widespread peer review by the
scientific community, have found that theses and dissertations may contain more, or
equivalently, stringent methodology than that found within published studies (Hopewell,
McDonald, Clarke, & Egger, 2007; McLeod & Weisz, 2004). Whilst any form of unpublished
academic literature might be considered to be grey literature, theses and dissertations have the
advantage of undergoing peer review from a (albeit, small) number of reviewers. Therefore, it
would seem that unpublished theses and dissertations have the capacity to reduce publication
bias, whilst maintaining methodological quality, and strengthen the empirical base into
populations for which there is a paucity of research. In this way, a systematic review supports
clinicians and researchers to benefit from the synthesis of a greater wealth of research where bias
is minimised to support translation into clinical and academic practice.
Evaluation of the methodological stringency of ACT research may be particularly salient, as a
previous systematic review and meta-analysis of the adult literature, concluded methodological
concerns are more typical in ACT research than in traditional CBT and that ACT did not met the
requirements to be an “empirically supported treatment” (Ost, 2008). However, the conclusions
of this review are not without contention. Gaudiano (2009) argued that the strategy utilised by
Ost to compare methodological quality of ACT and CBT was mismatched, with the majority of
ACT studies conducted among populations widely acknowledged to be treatment-resistant. ACT
and CBT were also noted to be at markedly different stages of clinical trial research and
associated grant support, favouring CBT, which was moderately correlated with methodological
rigour (Gaudiano, 2009). Whilst this review was not without criticism, Ost was commended for
attempting to evaluate the methodological stringency of the literature when making conclusions
on its applicability for clinical practice (Gaudiano, 2009).
In summary, whilst two previous reviews of ACT for children have been conducted, these are
subject to several limitations including non-scientific approaches and the inclusion of studies that
are purely theoretical or not subjected to peer-review. At the time of the publication of the most
recent review, few empirical studies had been conducted and those that were available were
predominantly case studies or uncontrolled pilots (Coyne et al., 2011). In the past few years the
ACT literature has seen a proliferation of studies involving child and adolescent populations. As
an increasing number of studies are now available there is a growing need for a systematic
review of the utility of ACT for children. The current investigation aims to address this gap in
the literature by providing an integrated synthesis of both the published and unpublished
literature for ACT in the treatment of children that incorporates both an exploration of findings
and an evaluation of the methodological rigour of included studies. The diverse literature will be
synthesised to elucidate generalisations, consistencies and inconsistencies in research findings to
enable evidence-based clinical decision-making in this area and minimise bias (Higgins &
Green, 2011; Mulrow, 1994). The analysis of the methodological rigour of included studies will
also offer ecological validity information to assist clinicians in translating research into practice.
To the authors’ knowledge, this is the first systematic review to specifically focus upon children.
Method
Search and screening procedures
Electronic searches of the PsycInfo and PsycArticles and PsycExtra databases were undertaken
to obtain the published literature. Whilst no date restrictions were employed, the search was
conducted in December 2014 and therefore included literature available up to this time.
Considered to be an international online learning and research community for researchers and
clinicians with an interest in ACT, the Association for Contextual Behavioral Science webpage
(http://contextualscience.org/) was also searched, for the same time period. To minimise
potential publication bias, a search of the unpublished literature was undertaken via the Proquest
dissertations and theses database, up to December 2014. Search terms used were “Acceptance
and Commitment Therapy” AND “child*”, or “adolescen*”, or “teen*”. Manual searches of
reference lists were conducted for each included study, followed by citation searches to locate
additional studies for inclusion. The title and abstracts of citations attained from initial searches
and via secondary examination of reference lists were subjected to the below inclusion and
exclusion criteria by the first two authors. Where there was disagreement on eligibility, the study
was jointly reassessed by both authors to achieve a unanimous result. In the event that this could
not be reached, the third author was available to make a determination. Full papers of retained
citations were retrieved and re-subjected to the below full inclusion and exclusion criteria.
Inclusion criteria
Inclusion criteria for the current review included:
a) Intervention studies of ACT or studies that employed a minimum of two of the ACT
hexaflex processes: mindfulness, acceptance, cognitive defusion, self-as-context,
values and committed action.
b) Studies that treated child participants up to age 18 years
c) Articles prepared in English
Exclusion criteria
a) Review, meta-analysis or theoretical articles
b) Studies that lacked at least one psychometrically validated measure
To enable maximum breadth of the review no inclusion restrictions were placed on study design,
disorder or problem of interest, setting, or control/comparison condition or timeframe to follow-
up.
Eligible studies
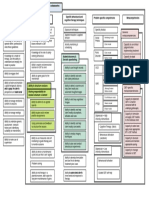
The initial search identified 169 citations (following de-duplication). An examination of
reference lists produced an additional 33 citations. Of these 202 citations, 33 met initial inclusion
criteria. Full papers were retrieved for these 33 citations. See Figure 1 for an overview of the
study selection process.
<insert figure here>
Figure 1. Selection of studies
Twenty papers met full inclusion criteria, detailing 21 unique studies. The first two authors were
unanimous with respect to eligible studies. The reasons for exclusion of the 13 papers that met
initial inclusion criteria, but were excluded after full review, are summarised in Appendix A. The
primary reason for exclusion at this stage related to the paper not reflecting an intervention trial
(i.e. theoretical papers or reviews etc.).
Data extraction, synthesis and quality assessment
Data was extracted to a standardised coding sheet for all studies meeting inclusion criteria. Data
extracted included population characteristics, setting, disorder/concern being treated, research
design, treatment conditions, treatment duration and outcomes. Outcomes of interest included: 1)
reductions in clinician-rated, parent-rated, self-reported or objective measures of a) symptoms
and/or b) QOL outcomes and/or c) psychological flexibility and; 2) maintenance of treatment
gains at follow-up. Due to the heterogeneity of studies and few with reported effect sizes, this
evaluation is limited to a narrative synthesis.
As heterogeneity of the sample studies was expected, it was important to assess methodological
quality to account for likely confounding factors. Quality assessment was conducted using the
22-item “Psychotherapy outcome study methodology rating form” (POMRF) devised by Ost
(2008). As discussed, the Ost (2008) review has some limitations, but his methodological
critique using the POMRF has been acknowledged as an important step in progressing the field
(Gaudiano, 2009). The POMRF includes 22 methodological components such as sample
characteristics, the psychometric properties of outcome measures, research design, controls,
therapist training and therapeutic modality adherence. Each item is rated on a 3-point scale
where 0 = Poor, 1 = Fair, and 2 = Good. Each study receives an overall score between 0 and 44,
with higher scores indicative of greater methodological rigour. The POMRF has good internal
consistency (0.86) and interrater reliability within the range 0.50–1.00 with a mean of 0.75 (Ost,
2008). Quality assessment data were extracted by the first two authors to a second coding sheet
developed for this purpose. Where quality assessment judgement was subject to discrepancy the
study was jointly reassessed by the two first authors to gain a unanimous result. Where this could
not be reached the third author was available to make a determination.
Results
Overview of included studies
Table 1 provides an overview of included studies. Studies included a total of 707 participants and
incorporated treatment for children with anorexia nervosa, depression, pain, trichotillomania,
sickle cell disease, tic disorders, obsessive-compulsive disorder, anxiety symptoms,
posttraumatic stress disorder (PTSD) / posttraumatic stress symptoms (PTS),
impulsivity/problem/sexualised behaviour, self-harm, stress symptoms, emotional dysregulation,
Aspergers Syndrome, and attention deficit hyperactivity disorder. Eighty percent of the studies
were published journal articles and the remaining 20% were made up of unpublished university
theses or dissertations.
Sample characteristics
Pain was the most commonly investigated condition (n=5; 23.81%) and studies employed
predominantly clinical outpatients (n=16; 76.19%). The sample size ranged from 1 to 339
participants. Overall, studies were relatively gender balanced. Participants ranged in age from 6
to 18 years, with the majority of studies conducted with adolescents (>11 years; n=17; 80.95%),
compared to younger children (<12 years; n=4; 19.05%).
Study design and treatment conditions
There were seven within-group designs (33.33%), six case studies/series (28.57%), four
between-group designs (19.04%; with two including control conditions), and the same
proportion of RCTs. The majority of studies involved individual treatment (n=14; 66.67%), with
a lesser proportion undertaken in group format (n=5; 23.8%). One was a family-based
intervention, and another did not specify the treatment format (4.76%). High heterogeneity was
observed in terms of treatment duration, with studies ranging between 5-90 hours.
Control/active comparison and random assignment
A large proportion of studies did not utilise a control comparison group (n=10; 47.62%). Of the
eleven studies that did employ a control group, five (23.8%) used a treatment-as-usual (TAU)
comparison. Two studies (n=2; 9.52%) utilised multiple baseline and, another two, baseline
control. One study employed a waitlist control, and another one did not specific the form of
control employed (4.76%). One study compared ACT with another active treatment, habit
reversal training. Overall, only the four RCTs utilised random assignment of participants to
treatment, with one further Australian study employing a random allocation for female, but not
male participants (Livheim et al., 2014).
Assessment of methodological quality
Significant variability in methodological rigour was evident with overall POMRF scores ranging
from 3-25 out of a total of 44 points, with the average score 13.29 (SD = 5.12; Table 2). As Ost
(2008) did not include cut-off scores for the POMRF, standard deviations (SD; rounded to the
nearest whole number) were utilised to attain a POMRF rating in order to compare studies, in
line with an earlier systematic review of ACT in the treatment of anxiety (Swain, Hancock,
Hainsworth, & Bowman, 2013). Swain et al. (2013) rated studies more than one SD below the
mean POMRF score “well below average” (current investigation range 0–7), those within one
SD of the mean “below average” (8-13), “above average” (14-18), and “well above average”
(19+). See Table 2 for POMRF scores and ratings.
Many methodological components were ignored by the studies in this review and where studies
did address a component, this was typically done to a “fair”, rather than “good” standard. One
study (4.76%) described a power analysis and two employed blind evaluators (9.52%). Four
studies (19.05%) incorporated adequate controls for parallel treatment completed external to the
research; all at the fair standard. Four (19.05%) involved a comparison to an alternative or well-
described TAU condition and the same proportion evaluated the clinical significance of findings.
Nine (42.86%) specified the assessors’ training or experience with the assessment tool employed,
with eight (38.1%) describing an approach for attrition handling. Whilst nine studies (42.86%)
provided information on the number of therapists involved in the intervention delivery, just one
did this to a good standard and 47.61% of studies provided some information about the
training/experience of therapists. Seven (33.33%) undertook treatment fidelity assessments and
whilst the same proportion examined therapist competence in the delivery of treatment, this was
done to a good standard by one study. Of the seven studies that compared ACT with another
active treatment or TAU, inequity of therapy hours was common, with only one study attaining a
“fair” rating for this item (14.29%). Studies performed better in terms of assessment time points,
with 20 (95.24%) detailing fair-to-good use of reliable outcome measures. Thirteen studies
(61.9%) included at least three rounds of assessment and over 95% of studies (n=20) had fair-to-
good specificity of measures as well as a specified treatment protocol. Finally, 15 studies
(71.43%) provided a fair-to-good description of the participant sample.
Outcomes
Study outcomes are depicted in Table 2. Where data from multiple assessment points was
reported, these are delineated by a backslash (/). While few studies reported effect sizes (ES),
reliable change or clinically significant change indices, these are reported where available. A
narrative synthesis of these results ordered by POMRF rating, from most to least rigorous
methodological category follows.
Well above average
Three studies (14.29%) were rated as well-above average in terms of methodological rigour.
These included two RCTs (L. Hayes, Boyd, & Sewell, 2011; Metzler, Biglan, Noell, Ary, &
Ochs, 2000) and one between-group study (Franklin, Best, Wilson, Loew, & Compton, 2011).
The utility of a behaviour therapy program (including ACT approaches) versus TAU
(psychoeducation) for 339 adolescents with high risk sexualised behaviour was examined in one
study (Metzler et al., 2000). At 3-month follow-up, in contrast to predictions, ACT participants
engaged in greater frequency of sex than TAU participants. At 6-month follow-up, ACT male
participants reported significantly fewer partners than TAU males, but not females. Relative to
TAU, ACT participants reported significantly fewer instances of, and improvements in, sexual
contact with strangers, as well as clinician-rated social competence. Limitations of this study
include low response (18%) and poor retention rate to follow-up assessment time points. The
sample also evidenced significantly higher risk taking behaviours than a random sample of
clients of STD clinics. Whilst this may cast doubt on the representativeness of findings, a
population exhibiting more problematic behaviours might be expected to be increasingly
treatment resistant, which lends further support for ACT. This may also explain the lack of
significant findings at the 3-month follow-up, as it may be that participants required more time to
consolidate therapeutic gains and generalise learnings to a greater number of behaviours. In
contrast to predictions, there were no significant between-group differences in acceptance
measures. However, this study was limited to assessment of acceptance alone and did not
account for the role of other proposed change processes within the ACT hexaflex. It is unclear
from this study the degree of experience of the treating therapists and this too may have impacted
on the findings, as has been identified in other studies (e.g., Franklin et al., 2011). Strengths of
this study include its sizable sample, treatment adherence checks and thorough analysis of
interaction effects. This study attained a POMRF score of 21/44.
In another RCT, 30 depressed adolescents were randomised to TAU (manualised CBT) or
individual ACT (L. Hayes et al., 2011). ACT resulted in significant improvement in depressive
symptoms at posttreatment and 3-month follow-up, findings of small and large effect sizes,
respectively (L. Hayes et al., 2011). Clinically reliable change was observed among 58% of ACT
participants and 36% of TAU participants. ACT achieved greater reductions in depressive
symptoms than TAU at posttreatment and follow-up. At posttreatment and follow-up, 26% and
38% of ACT participants showed reliable clinically significant improvement. Strengths of this
study included the use of trained therapists and psychometrically validated instruments.
Therapists in this research were involved in the delivery of both ACT and TAU interventions,
but a limitation of this study included a lack of information regarding treatment duration, and
treatment fidelity or therapist adherence, preventing examination of contamination of treatment.
This is important as, to draw meaningful conclusions about the effectiveness of treatment,
treatment must be delivered as per protocol (Ost, 2008). The POMRF for this study was 20/44.
Franklin et al. (2011) undertook a trial of habit reversal training (HRT; n=7) versus ACT+HRT
(n=6) among adolescents with chronic tic disorders. Results revealed significant reductions in tic
severity across treatment, with no significant differences between groups. However, in terms of
clinician-rated global impression ratings, superior outcomes were observed for HRT relative to
ACT+HRT in terms of overall percentage improved at each time point (43% vs 40% at week 10;
86% vs 25% at week 14; 57% vs 20% at week 18 and; 71% vs 33% at one-month follow-up).
Likewise, although no statistical comparisons were made on self-rated functioning, a visual
inspection of scores suggested HRT performed somewhat better than ACT+HRT. Strengths of
this study include the use of validated diagnostic instruments, trained assessors who were blind
to treatment allocation and trained therapists. This was the only study included within this
review that compared an ACT protocol with another active alternative treatment and it received
the highest POMRF score in this investigation (25/44). However, a larger sample would have
increased the power to enable further statistical analysis and detect significant effects. All but
one of the therapists involved in this study were relatively inexperienced in ACT and had greater
experience in HRT, which may have implications for treatment quality. In line with this
assertion, the more experienced therapist in this study was found to achieve more substantial
reductions in tic severity scores than did those therapists with minimal experience.
To date, among the child literature, the best evidence for ACT exists for the treatment of tic
disorders, depressive symptoms and high risk sexual behaviour. Taken together these offer
preliminary evidence for ACT in improving both self and clinician-reported outcomes. However,
some improvements were not observable until follow-up, and others observed larger
improvements some months after therapy cessation. ACT was superior to TAU in both studies
that employed these comparisons, which suggests its utility for clinician treating children with
these concerns. While, for chronic tic disorders the addition of ACT to HRT did not produce
additional gains, more experienced ACT clinicians were found to achieve improved outcomes
relative to those with less training. Limited evidence is currently available in the most
methodologically rigorous studies on changes in the ACT core processes.
Above average
Seven studies (33.33%) attained above average ratings on the POMRF. Two examined the
effectiveness of ACT for OCD among three children aged 10-13 years (Armstrong, 2011;
Yardley, 2012). Armstrong (2011) found mean compulsion scores decreased 28.2% on clinician-
rated and 40.4-64.5% on self-reported measures. All participants showed improvement across
measures, with two participants achieving subclinical scores at posttreatment. In line with this,
Yardley (2012) noted all participants showed large improvements across clinician-rated
measures, reflecting an average drop of 47.26%. Self-reported obsessive cognitions in two of
three participants also evidenced improvement. However, both studies are limited in small
sample size, representativeness of the sample, and non-report of control of external treatment or
therapist training. These factors limit the applicability of findings.
The utility of ACT for PTSD/PTS was examined among a mixed sample of community-dwelling
adolescents with PTSD/PTS and adolescent inpatients with PTSD/PTS and a comorbid eating
disorder (Woidneck, Morrison, & Twohig, 2014). Results indicated reductions in the frequency
and intensity of self-rated PTSD/PTS symptoms at posttreatment, reflecting reductions of 63-
69% and 59-81% for the community and inpatient participants, respectively. Similar rates were
found at 3-month follow-up. On clinician-rated measures at posttreatment the average reductions
were 57% and 61% for the community and inpatient participants, respectively, with 71% and
60% at the 3-month follow-up. Avoidance and fusion significantly decreased at posttreatment by
an average of 65% for the community and 57% for the residential participants, with further
reductions at 3-month follow-up. Statistical analysis of QOL outcomes was not reported;
however, visual inspection of raw scores on these measures suggested improved QOL at
posttreatment, with gains maintained or further improved at 3-month follow-up. The small
sample size and the mixed participant sample limits the generalisability of the findings, which
may have impeded a statistical comparison between the residential and community participants.
This is particularly salient as the former were also receiving intensive TAU in the residential
environment for their primary diagnosis of eating disorder. As such, it is difficult to determine
whether TAU may have been diluting the effects of ACT. The therapist was also known to the
residential participants, prior to their commencing ACT treatment and therefore rapport levels
were likely between the groups and this may have impacted on obtained findings. The lack of
independent assessors in this study also may have introduced a degree of bias to the research, as
the therapist also completed all assessments. The resultant POMRF score for this study was
16/44.
An ACT-based group therapy was examined among 28 children presenting with, or at risk for,
emotional dysregulation and externalizing behaviour (Bencuya, 2013). The sample included
children adopted from foster care (n=24), with a lesser proportion (n=4) non-adopted. Forty-two
percent were medicated for psychiatric concerns. At posttreatment, parent-rated measures of
child emotional avoidance, behavior problems, internalizing problems (trend only), and ADHD
symptoms had significantly reduced. Among non-medicated participants, parent-rated child
metacognition deficits decreased and executive functioning was not significantly different.
Among medicated participants, metacognition deficits had increased. Among child-reported
measures there were no significant differences on cognitive emotion regulation or mindfulness at
posttreatment. At follow-up, child-reported cognitive emotion regulation, mindfulness, and
avoidance/fusion significantly improved, relative to pretreatment. Limitations of this study
include the diverse nature of the sample as well as the unequal distribution of participants to
condition. The latter may explain the lack of significant findings between participants in the
waitlist and immediate treatment conditions. This study achieved a POMRF score of 14/44.
Wicksell, Melin, Lekander, and Olsson (2009) compared an ACT-based intervention with TAU
(multidisciplinary plus medication approach) among 30 children with mixed idiopathic pain.
ACT produced significant improvements of small effect size across all primary outcome
measures (pain-related functioning, impairment, interference and health-related QOL) over time
(up to 6 months post). The TAU group also improved across primary outcome measures with the
exception of mental health-related QOL. At posttreatment ACT outperformed TAU on pain
measures and mental health-related QOL. Incorporating all time points, ACT evidenced superior
outcomes to TAU on pain outcomes. Limitations in the current study included a disproportionate
number of sessions across condition (13 ACT versus 22.8 TAU), and the use of outcome
measures with unknown psychometric properties, not validated among young people. The
sample were also highly diverse in terms of clinical presentations, as well as duration of
condition and treatment history, which may have implications for external validity. The
methodological quality of this study was rated as 17/44.
Another study among adolescents experiencing chronic pain observed functional disability and
school absenteeism improved by 63% and 68%, respectively, at posttreatment (Wicksell, Melin,
& Olsson, 2007). Pain intensity and interference were reduced by around 50%. Gains were
maintained at follow-up. Changes were clinically significant for over 70% at posttreatment and
all but one participant at 3-month follow-up. At 6-month follow-up all participants evidenced
clinically significant decreases in pain interference, with 73% for intensity. At posttreatment
there were significant decreases in internalising/catastrophizing, maintained at follow-up.
Caveats of this study include the diverse nature of the sample and the sample size, which limits
the generalisability of findings. Treatment also varied in terms of length and focus with respect
to individual therapeutic goals. Although broadly reflective of clinical practice this lack of
standardisation may have implications for the external validity of findings.
Livheim et al. (2014) detailed two pilot studies, completed over two countries, to examine the
effectiveness of a manualised group ACT program for adolescents with depressive symptoms
(Australian study; N=66) and stress symptoms (Swedish study; N=32). The Swedish study
achieved POMRF rating in the above average range, whereas the Australian study scored in the
below average range. In the Swedish study, participants were randomised to ACT or TAU
individual counselling with the school nurse. At posttreatment a large significant improvement
was observed in self-reported perceived stress in favour of ACT, with no change for TAU. No
significant differences were observed in self-reported QOL, depression, stress, anxiety
(marginally significant improvement relative to TAU) or general mental health. Change in
avoidance and fusion was non-significant, with change in mindfulness marginally significant for
ACT relative to TAU. Greater session attendance was associated with significantly higher QOL
ratings and improved depression and stress ratings. Limitations specific to this study included
that the TAU intervention was completed in individual, not group format, and was not
administered to all participants or in a consistent fashion. This inequity in the comparison makes
it difficult to delineate the impact of factors such as the delivery format or therapeutic hours in
contributing to the outcome. Whilst this study reported a power analysis, the number of
participants was less than anticipated and as a consequence, it was underpowered. Thus, it is
possible that significant effects that may have been present were not detected. This study attained
a POMRF of 14/44.
Taken together, studies with above average methodological rigour showed ACT to be effective
in achieving reductions in clinical and self-rated OCD, pain symptoms, and PTS/PTSD, at
posttreatment and follow-up. Pain and OCD outcomes were consistent across two studies.
Among children experiencing or at risk for emotional dysregulation ACT was also effective in
improving the majority of parent-rated measures at post and follow-up. However changes in
child-ratings were not apparent until follow-up. Mixed findings were observed for the
effectiveness of ACT among children with stress. However this study was also underpowered,
which may have impacted on findings. QOL outcomes were examined in one study on pain and
one on stress. The former found significant changes over time and relative to TAU for ACT, in
the latter changes were non-significant. Concerning ACT process measures, avoidance and
fusion significantly reduced among children with PTS/PTSD as well as those experiencing or at
risk for emotional dysregulation.
Below average
In accordance with POMRF ratings, eight (38.1%) studies scored below average. The utility of
ACT as a treatment for trichotillomania was examined in a case series of two adolescents (Fine
et al., 2012). While both participants evidenced decreases in focused and automatic hair pulling
over the course of 11 treatment sessions, methodological caveats included a lack of therapist
training information, checks for treatment adherence/therapist competence and an absence of a
follow-up assessment. As a case study it also lacked a control group and random allocation to
treatment, it attained a POMRF rating of 8/44.
The second of the pilot studies described by Livheim et al. (2014) was completed with Australian
adolescents with depressive symptoms (N=66). This study employed a planned comparison,
where girls were randomised to ACT or TAU (12-weeks monitoring by school counsellor), and a
single boys group (N=8) received ACT. Significant improvements of large effect size in self-
reported depression overall were observed among ACT participants, with no changes for TAU,
at posttreatment. Effects favoured ACT across the dysphoric mood, anhedonia/negative affect
and negative self-evaluation symptoms, with moderate to large effect sizes. No significant
changes were observed on somatic symptoms. Changes in acceptance and defusion were only
marginally significant for ACT relative to TAU. Caveats included the non-measurement of
participant session attendance, which affects measurement bias. Pretreatment differences in
overall depression scores were observed and thus an alternative interpretation of effects may be
that changes reflected a regression to the mean (i.e., if a variable is extreme on its first
measurement, it will tend to be closer to the average on its second measurement). Other
limitations of this study included the sole reliance on self-report measures, which are impacted
by social desirability. The vast majority of participants were female, which impacts on the
capacity to generalize the result to male populations. Follow-up assessment was not included to
examine the durability of observed outcomes. This is important as other studies with children
have found that the effects of ACT are not immediately observable at posttreatment. Finally
therapist competence and adherence to the protocol were not examined. Given the therapists
were relatively inexperienced in the use of ACT this is an important consideration in determining
whether the program was ACT consistent.
In a study on chronic pain and ACT, 20 children evidencing moderate functional disability from
chronic pain were allocated to ACT (N=10) or to an undefined control condition (N=10)
(Ghomian & Shairi, 2014). Both child and parent reports in the ACT group evidenced significant
changes in overall functional disability as well as the capacity to perform physical and daily
activities. There were no significant changes for controls. Parent reports indicated ACT
outperformed control across outcomes at posttreatment and 1.5 month follow-up. Relative to
pretreatment, at 3 month follow-up parent reports indicated significant differences in favour of
ACT, relative to control, on both routine and total functional disability. Gains were maintained
between posttreatment and follow-up. On child-reported physical disability there were no
significant differences between ACT and control across time, in contrast to parent-reported
outcomes. However, the quality of this study is weakened by its reliance on one outcome
measure. Furthermore, the limited detail on the treatment protocol in makes it difficult to
determine the methodological rigour of the research (e.g., whether the treatment was delivered in
individual or group format, etc.), reflected in its POMRF score of 10/44.
Another study on pain involved a three week group-based interdisciplinary residential program
with 98 adolescents (Gauntlett-Gilbert, Connell, Clinch, & McCracken, 2013). The program
consisted of physical conditioning, activity management, and ACT approaches. Results showed
improvements at posttreatment, of small to medium effect sizes, in school attendance,
medication and health care usage, acceptance, pain anxiety, depression, catastrophizing,
social/physical functioning, development, and objective physical measures. Pain intensity did not
change, in contrast to the observations of Wicksell et al. (2007). At follow-up, all measures
significantly improved except pain intensity, depression, and development. Increased acceptance
was related to improved physical and social functioning, objective physical measures, and all
psychological variables. There are several limitations of this study, reflected by its POMRF score
(11/44). The lack of a control group and the use of an interdisciplinary multicomponent approach
may confound the extent to which changes in measures can be attributed to ACT. This may also
explain the differences in pain intensity to that of Wicksell et al. (2007). However, as stated by
the authors, results were consistent with the ACT model, in that changes occurred in functioning,
in the absence of similar reductions in pain outcomes (Gauntlett-Gilbert et al., 2013). Other
caveats include the lack of treatment adherence or fidelity evaluations and difficulties of
generalizing the results from intensive residential treatment to other settings. Furthermore, this
study examined associations between changes in one ACT process measure, acceptance, and
other outcomes, and did not examine the remaining ACT hexaflex processes, despite their
inclusion in treatment. As a consequence it is unclear how these might be differentially related to
changes in other measures.
Heffner, Sperry, Eifert, and Detweiler (2002) examined ACT in the treatment of a 15 year old
with anorexia nervosa. Results showed ACT produced movement from the clinical to nonclinical
range at treatment cessation on drive for thinness and ineffectiveness outcomes. However, a
body dissatisfaction measure, remained within the clinical range. The participant’s weight fell
within the normal range at follow-up, and typical menstruation resumed. The methodological
quality of this study was below average (9/44), reflective of the case design and ensuing
limitations as well as lack of treatment adherence checks.
A group-based ACT protocol was examined in a group of seven adolescents with Asperger’s
Syndrome and/or non-verbal learning disability (Cook, 2008). At posttreatment significant
improvements in valued living were observed, but changes in avoidance and fusion were
nonsignificant. Correlations between change scores on avoidance/fusion and obsessive-
compulsive, interpersonal sensitivity, depression, anxiety, hostility, paranoid ideation, and
psychoticism measures were observed (Cook, 2008). Limitations of this study include the small
sample, the absence of control comparison, sole reliance on self-report measures and a lack of
statistical analysis of changes. The level of experience of the graduate student facilitator with
ACT was unclear and treatment fidelity/adherence checks were not in place to ensure
consistency with the protocol. This study scored 12/44.
Another study examined the utility of an acceptance and mindfulness “self-control training”
intervention for three children with ADHD (Seibert, 2011). Following baseline stabilization,
associated with time tolerated before eating a preferred food, all participants underwent five
sessions of self-control training. This involved learning acceptance and mindfulness skills in
response to impulsive thoughts and bodily sensations evoked in the desire to eat a preferred food.
At the conclusion of each of the five sessions, participants had access to a preferred food after a
delay period of 10 times their baseline time. As predicted, all participants were able to tolerate a
greater delay after self-control training and could meet the 10 times time requirement for self-
control training for the majority of training sessions. Two of three participants met this for 100%
of self-control training trials, and the third participant for all but one trial. Two of three
participants tolerated three times their natural baseline delay to receive a large portion of their
preferred food. One participant continued to be unable to tolerate this delay. Limitations of this
study included the small sample, lack of control group, absence of reliability checks of diagnoses
and therapist competence. Treatment involved only two of the six ACT core processes, which
limits conclusions about the utility of ACT more broadly. In line with these caveats, this study
received 12/44 on the POMRF.
In another study, 15 adolescents with high self-reported problem behaviours completed a
program that included three core processes of the ACT hexaflex; values, cognitive defusion and
self-as-context (Luciano et al., 2011). The study trialled a values intervention with either
defusion (Defusion I) or defusion + self-as-context approaches (Defusion II). On the basis of the
number of endorsed problem behaviours, participants were classified as high (score 6) or low
risk (scores 5). Half of the low-risk participants received Defusion I. The remaining half of the
low-risk, and all high-risk participants, received Defusion II. All participants received the values-
orientated session. There were significant changes in problem behaviours and differences
between groups subsequent to the values-orientated session. For Defusion I no significant
differences were observed for measures of problem behaviour, experiential avoidance/fusion or
acceptance across time. Low-risk participants in Defusion II evidenced significant changes
across all measures with results maintained at follow-up. Four of five participants reported no
problem behaviour at post and maintained this at follow-up. Results for high risk participants
were equivalent, with two exceptions; experiential avoidance/fusion did not change over time,
and improvements in acceptance at post were not maintained at follow-up. A comparison among
low risk participants across defusion conditions revealed consistently significantly superior
results for Defusion II. The authors concluded that defusion was bolstered by the inclusion of
self-as-context approaches. The lack of changes in avoidance/fusion among high risk participants
was unexpected. It is possible that the intervention was of insufficient duration to evidence
changes on this measure among participants with more severe behavioural problems. This study
was limited by the overall numbers in each group, and use of only three of the six core ACT
processes. Given the low number of studies in this category and the low sample sizes used, this
study scored 12/44. Further studies to examine the comparative effectiveness of ACT are
warranted.
Studies scoring one standard deviation below the mean POMRF rating for methodological rigour
found that ACT was effective in reducing the majority of self-reported clinical outcomes among
participants with trichotillomania, depression, pain (two studies), anorexia, ADHD, and problem
behaviour. Results were also consistent on parent-report in one study of children with pain
conditions. Where ACT was compared with TAU, ACT achieved favourable clinical outcomes
among participants with depression and pain, across time. With respect to process measures,
changes in avoidance and fusion were mixed. Improvements were found among children who
endorsed five or less problem behaviours, but not among those with six or more, and non-
significant changes were observed among adolescents with Asperger’s Syndrome. Acceptance
improved among participants in one study of children with pain conditions and among those with
problem behaviours. Significant improvements in valued living were observed among children
with Asperger’s Syndrome.
Well below average
Three studies (14.29%), all case studies, scored well below average on the POMRF. By their
very nature, case-studies are limited in their ability to determine whether change observed was
greater than chance alone. Their sample size also makes generalisation of the findings difficult.
However, these studies make an important contribution to the field in that it supports the clinical-
research community by providing data on a population for which there is a dearth of research.
Disorder and treatment-tailored studies such as those explored in these case studies and the
ability to draw conclusions from research conducted in naturalistic settings is often not possible
in large efficacy studies, thus case-studies are often a necessary precursor to appropriately
designed larger-scale trials.
A study of ACT for a 14-year-old female with idiopathic pain found reductions in functional
disability, pain and emotional-focused avoidance at posttreatment (Wicksell, Dahl, Magnusson,
& Olsson, 2005). Improved school attendance and achievement of values-based goals was also
observed with results maintained at follow-up. This study received a 7/44 POMRF rating, a
reflection of its case study nature, lack of treatment adherence and competence checks, and
reports of clinical significance.
Brown and Hooper (2009) examined ACT in the treatment of anxiety in an 18 year old female
with a moderate-to-severe learning disorder and school refusal. Experiential avoidance had
reduced at posttherapy. The participant was increasingly calm and socially confident, and had
recommenced school in accordance with anecdotal parent-report. Gains were maintained at
follow-up. However, several caveats limit the generalisability of findings, reflected in its
POMRF score of 3/44, the lowest of all studies included within this review. One
psychometrically evaluated assessment tool was employed, focused on ACT processes of
change, and this study relied on anecdotal evidence to determine the impact of treatment on the
clinical outcome of anxiety severity. The intervention was markedly different from protocol, as
therapeutic adjustment were made throughout and the program extended extending beyond the
proposed 10 session to a 17 session intervention.
A family-based ACT intervention was completed with a 16 year old male with sickle cell disease
(SCD) who experienced pain, fatigue, social apprehension and adaptive behaviour deficits in
studying, socialisation and inattentiveness/inaction (Masuda, Cohen, Wicksell, Kemani, &
Johnson, 2011). No significant self-reported changes in social anxiety or QOL were observed at
posttreatment, although scores remained in the normal range relative to a comparative sample of
SCD children. However, at follow-up, social anxiety and QOL scores improved to one standard-
deviation below and above, respectively, the average in the comparison sample. Pain reports
remained unchanged over time. Parent-report indicated improvements academic performance
and functioning. Scores on avoidance/fusion were greater than the comparison sample at pre and
posttreatment, however, large reductions were observed at 3-month follow-up. The case study
nature of this study, lack of report of assessor training and treatment adherence/fidelity, are
reflected in its POMRF score of 7/44.
In summary, two of these studies examined changes in clinical outcomes, with both observing
improvements in self and parent reported outcomes. These studies showed some support for the
processes of committed action, via the achievement of values-based goals, as well as
improvements in avoidance and fusion at either post or follow-up. As described above, these
studies should be interpreted with caution, given their methodological limitations. However,
clinicians working with children exhibiting less prevalent conditions such as SCD or those
working in disability settings may glean some utility from these findings for their populations.
Discussion
The past few years has seen a proliferation of ACT research in the treatment of conditions among
children. While there are two existing reviews of the literature, the present investigation is the
first to be conducted systematically. It involved both the published literature as well as
unpublished theses/doctoral dissertations and specifically targeted studies involving treatment for
children, rather than parent-based interventions. It also expands upon the findings of earlier
reviews through an update of the literature completed over the past few years and the inclusion
of a greater number of intervention-specific studies.
Twenty-one eligible studies were identified involving treatment for a spectrum of presenting
issues. While the literature is still in its infancy, and subject to several methodological quality
issues, the evidence available to date suggests that ACT produces significant improvements in
the majority of self and clinician-reported clinical outcomes across presenting problems. While
few studies incorporated parent-reported outcomes, where these were used, they were broadly
consistent with child and clinician-rated outcomes. These findings support the argument of
several researchers (e.g., Coyne et al., 2011; Greco et al., 2005; Hadlandsmyth et al., 2013) who
suggest that ACT is a viable therapeutic approach for clinicians working with child populations.
These outcomes also support the assertion that ACT has potential utility as a transdiagnostic
approach (S. C. Hayes et al., 2012; Livheim et al., 2014), an area for future research in larger,
methodologically rigorous trials with multiple clinical presentations.
There remains a relative dearth of comparisons of ACT to other active treatments. Just one study
included within this review, compared ACT to another active treatment, and found the addition
of ACT to another active treatment did not achieve more favourable outcomes (Franklin et al.,
2011). However, a key limitation in this study is that clinicians were relatively inexperienced in
the use of ACT, and expertise was associated with improved outcome (Franklin et al., 2011).
ACT can be rather counterintuitive for unfamiliar clinicians and it involves several experiential
exercises/metaphors that are abstract in nature. Arguably, this difficulty is intensified when
delivered to adolescents, a population who may exhibit a greater spectrum of
cognitive/development differences. Taken together, these findings implore the importance of
skill and competence in the use of ACT prior to attempting this approach with clients for optimal
outcomes.
More research is clearly warranted to establish whether ACT works better than alternative
approaches. Despite this limitation, those studies comparing ACT to TAU found ACT evidenced
superior outcomes among children with issues of pain, depression and sexualised behaviour. This
suggests ACT should be considered by clinicians working with children with these presenting
concerns and may achieve more optimal outcomes that typical treatments. Several studies found
that treatment gains were either not fully evident at posttreatment (or initial follow-up) or that
greater improvements for ACT were obtained some months after therapy cessation (e.g., L.
Hayes et al., 2011; Metzler et al., 2000; Wicksell et al., 2007). Thus the inclusion of follow-up
time points is an important consideration for future research.
Few presenting problems have been investigated among children by more than one or two
studies, and this is also important for future research to consolidate the evidence base. At this
stage the most widely researched condition is pain, with studies consistently observing that ACT
results in improvements in functional disability and interference. Although studies differed in
methodological rigor, outcomes were consistent in this area. Thus, there is encouraging support
for clinicians to employ ACT approaches with young people presenting with pain concerns.
However, as the majority of these studies were conducted by a group of affiliated researchers
possible author bias cannot be ruled out. As such, it is recommended other researchers in
different settings test and replicate these findings. This links in with the concept of therapist
allegiance, which potentially affects outcomes in psychotherapy research. For instance,
allegiance bias may occur with study results being contaminated or distorted by the
investigators’ preferences towards a treatment or theory (Luborsky, Singer, & Luborsky, 1975).
In a meta meta-analysis of 30 meta-analyses (Munder, Brutsch, Leonhart, Gerger, & Barth,
2013) it was concluded that the researcher alliance outcome association is substantial and robust.
For example, a researcher’s enthusiasm towards a therapy might result in superior training and
supervision of the therapists implementing that treatment, as opposed to a less preferred
comparative treatment. It is also possible that greater experience and skill in a preferred
treatment could, however inadvertently, result in better performance of this treatment over a non-
preferred intervention. Thus the importance of reporting allegiances and considering the potential
for such bias to occur should be addressed in future research.
Despite the focus of ACT on QOL outcomes, few studies included within this review examined
changes in QOL specific measures. Thus, the research base is currently limited in the ability to
draw meaningful conclusion on the impact of therapeutic changes on children’s day-to-day
living. Future research should augment clinical outcomes with those specific to QOL, which
have been argued to reflect the clinical significance of changes (Gladis, Gosch, Dishuk, & Crits-
Christoph, 1999; Kazdin, 1977; Safren, Heimberg, Brown, & Holle, 1996). Studies that did
employ these measures all found improvements over time, with the exception of the study on
stress (Livheim et al., 2014), which was underpowered to detect effects. In line with findings on
clinical outcomes, the latter study observed superior outcomes among ACT participants, relative
to TAU. Taken together, these findings offer preliminary evidence for the utility of ACT in
improving both clinical and QOL outcomes among children.
Limited evidence is currently available on changes in the ACT core processes among children,
particularly in the most methodologically rigorous studies, and the evidence available is mixed.
Avoidance and fusion was the most commonly investigated process. Among eight studies 50%
indicated improvements at post or follow-up. Others observed a nonsignificant positive trend
(Cook, 2008), found improvements were limited to presentations of lower severity (Luciano et
al., 2011) or saw no improvements (Livheim et al., 2014). Positive changes were observed in
acceptance across two studies, but not in a third, which was underpowered to detect effects.
Evidence for valued living and committed action was limited to one or two studies, with positive
improvements observed among participants treated with ACT. Investigation of the ACT core
processes is important due to their hypothesised role in increasing psychological flexibility.
Increased research effort in this domain is likely to support knowledge development into
processes through which ACT fosters positive outcomes, typically termed “the mechanisms of
change” (Ciarrochi, Bilich, & Godsell, 2010; Kazdin, 2007; Kraemar, Wilson, Fairburn, &
Agras, 2002). This in turn is likely to foster parsimonious clinical practice, optimising clinician-
patient encounters to facilitate shorter term interventions delivered with improved sensitivity and
specificity (Kazdin, 2007; Kraemar et al., 2002).
Overall methodological quality assessment identified a number of strengths among eligible
studies. Most employed sufficiently detailed treatment protocols as to allow for replication,
assessment of outcome was examined at follow-up time points, and most utilised specific
outcome measures that were also valid and reliable. Future research should continue to adhere to
these practices. However, several caveats were identified and should be addressed in ongoing
studies, including heterogeneity in treatment duration between groups and a lack of consideration
for the clinical significance of findings. Most studies did not report therapist training, checks for
treatment adherence or therapist competence. An effect size calculation was not possible in many
studies due to the methodological limitations such as low sample size. A comparison of average
POMRF ratings in the current investigation (M=13.29), relative to a recent review of ACT for
anxiety with predominantly adult studies (M=17.29; Swain et al., 2013) also suggests the
methodological quality of studies involving child samples presently lags behind that of the adult
literature. In explanation for this finding, there was a predominance of small heterogeneous
samples, few conditions were investigated by more than one study, and designs that typically
lacked control or alternative treatment comparisons, limiting conclusions. However, such studies
may offer greater validity for clinicians working in real-world contexts than randomised efficacy
trials due to the employment of naturalistic settings and multiple baseline measures. Thus the
contribution of case studies or those in naturalistic settings to the scientific body of knowledge
should not be disregarded, especially for clinicians working with children from low prevalence
clinical populations.
Areas needing investigating in future research include an examination of the role of demographic
factors in outcomes, as several studies found outcomes varied by factors such as gender and race,
and others still observed medication status was associated with divergent results. The expansion
of studies to children of different age groups and those experiencing comorbid problems, is also
indicated. Clinicians should note that there is currently a dearth of evidence for ACT among
children under 12 years and in ACT treatment delivered in group or family-based formats. In
many studies the ACT intervention employed was delivered as a component of a broader
intervention and thus it is difficult to determine the contribution of non-ACT therapeutic
components to outcomes. Findings must be replicated and examined relative to control
conditions as well as active treatment alternatives. For the majority of disorders/conditions
specific effectiveness is currently limited to one or two studies. Taken together, these findings
suggest such additional methodologically stringent research is warranted taking these observed
pitfalls into consideration. Despite the methodological inadequacies identified in the research
reviewed, it is encouraging to see the rate at which ACT research in children is increasing, as is
the scientific rigour.
Conclusion
Emerging research of ACT in the treatment of children is encouraging for the utility of this
therapeutic approach for clinicians working with young people. To consolidate and build upon
this preliminary evidence, larger methodologically rigorous trials are required across a broader
spectrum of presenting problems and particularly among younger children. As difficulties in
childhood can result in substantial impairment across various life domains, it is important that
appropriate, evidence-based, treatment is available. It is hoped that the results of this review will
support the conduct of future research in this area with increased methodological rigour, to
provide additional data on the utility of ACT as a viable intervention available to clinicians in the
treatment of problems among children.
References
AACAP. (2007). Practice parameter for the assessment and treatment of children and adolescents with
anxiety disorders. Journal of the American Academy of Child & Adolescent Psychiatry, 46, 267-
283.
AACAP. (2012). Practice parameter for the assessment and treatment of children and adolescents with
Obsessive-Compulsive Disorder. Journal of the American Academy of Child & Adolescent
Psychiatry, 51, 98 -113.
Arch, J. J., & Craske, M. G. (2008). Acceptance and commitment therapy and cognitive behavioral
therapy for anxiety disorders: Different treatments, similar mechanisms? Clinical Psychology:
Science and practice, 15, 263-279.
Armstrong, A. B. (2011). Acceptance and commitment therapy for adolescent obsessive-compulsive
disorder. Unpublished doctoral dissertation, Utah State University.
Bencuya, N. L. (2013). Acceptance and mindfulness treatment for children adopted from foster care.
(Unpublished doctoral dissertation), The University of California.
Blackledge, J. T., Ciarrochi, J., & Deane, F. (2009). Acceptance and Commitment Therapy :
Contemporary Theory, Research and Practice. Brisbane, QLD: Australian Academic Press.
Brown, F. J., & Hooper, S. (2009). Acceptance and Commitment Therapy (ACT) with a learning disabled
young person experiencing anxious and obsessive thoughts. Journal of Intellectual Disabilities,
13, 195-201.
Burke, C. A. (2010). Mindfulness-based approaches with children and adolescents: A preliminary review
of current research in an emergent field. Journal of Child and Family Studies, 19, 133-144
Chawla, N., & Ostafin, B. (2007). Experiential avoidance as a functional dimensional approach to
psychopathology: An empirical review. Journal of Clinical Psychology, 63, 871-890.
Ciarrochi, J., Bilich, L., & Godsell, C. (2010). Psychological flexibility as a mechanism of change in
acceptance and commitment therapy. In R. Baer (Ed.), Assessing Mindfulness and Acceptance:
Illuminating the Processes of Change. Oakland, CA: New Harbinger Publications, Inc.
Cook, S. (2008). Can you act with aspergers: A pilot study of the efficacy of acceptance and commitment
therapy (ACT) for adolescents with asperger syndrome and/or nonverbal learning disability.
(Unpublished doctoral dissertation), Wright Institute Graduate School of Psychology.
Coyne, L. W., McHugh, L., & Martinez, E. R. (2011). Acceptance and commitment therapy (ACT):
Advances and applications with children, adolescents, and families. Child and Adolescent
Psychiatric Clinics of North America, 20, 379-399.
Creswell, C., Waite, P., & Cooper, P. (2014). Assessment and management of anxiety disorders in
children and adolescents. Archives of Disease in Childhood, 99, 674-678.
Farchione, T. J., Fairholme, C. P., Ellard, K. K., Boisseau, C. L., Thompson-Hollands, J., Carl, J. R., . . .
Barlow, D. H. (2012). Unified protocol for transdiagnostic treatment of emotional disorders: A
randomized controlled trial. Behavior Therapy, 43, 666-678.
Fine, K. M., Walther, M. R., Joseph, J. M., Robinson, J., Ricketts, E. J., Bowe, W. E., & Woods, D. W.
(2012). Acceptance-enhanced behavior therapy for trichotillomania in adolescents. Cognitive and
Behavioral Practice, 19, 463-471.
Franklin, M. E., Best, S. H., Wilson, M. A., Loew, B., & Compton, S. N. (2011). Habit reversal training
and acceptance and commitment therapy for tourette syndrome: A pilot project. Journal of
Developmental and Physical Disabilities, 23, 49-60.
Gaudiano, B. A. (2009). Ost's (2008) methodological comparison of clinical trials of Acceptance and
Commitment Therapy versus Cognitive Behavior Therapy: Matching apples with oranges.
Behaviour Research & Therapy, 47, 1066-1070.
Gauntlett-Gilbert, J., Connell, H., Clinch, J., & McCracken, L. M. (2013). Acceptance and values-based
treatment of adolescents with chronic pain: Outcomes and their relationship to acceptance.
Journal of Pediatric Psychology, 38, 72-81.
Ghomian, S., & Shairi, M. R. (2014). The effectiveness of Acceptance and Commitment Therapy for
children with chronic pain on the function of 7 to 12 year-old. International Journal of
Pediatrics, 2, 195-203.
Gladis, M. M., Gosch, E. A., Dishuk, N. M., & Crits-Christoph, P. (1999). Quality of life: Expanding the
scope of clinical significance. Journal of Consulting and Clinical Psychology, 67, 320-331.
Greco, L. A., Blackledge, J. T., Coyne, L. W., & Ehrenreich, J. (2005). Integrating acceptance and
mindfulness into treatments for child and adolescent anxiety disorders: Acceptance and
commitment therapy as an example. New York: USA: Springer.
Hadlandsmyth, K., White, K. S., Nesin, A. E., & Greco, L. A. (2013). Proposing an Acceptance and
Commitment Therapy intervention to promote improved diabetes management in adolescents: A
treatment conceptualization. International Journal of Behavioral Consultation and Therapy, 7,
12-15.
Harris, R. (2009). ACT made simple: An easy-to-read primer on Acceptance and Commitment Therapy.
California: New Harbinger Publications, Inc.
Hayes, L., Boyd, C. P., & Sewell, J. (2011). Acceptance and Commitment Therapy for the Treatment of
Adolescent Depression: A Pilot Study in a Psychiatric Outpatient Setting. Mindfulness, 2, 86-94.
Hayes, S. C. (2004). Acceptance and Commitment Therapy, Relational Frame Theory and the third wave
of behavioural and cognitive therapies. Behavior Therapy, 35, 639-665.
Hayes, S. C., Levin, M., Plumb-Vilardaga, J., Villatte, J. L., & Pistorello, J. (2013). Acceptance and
Commitment Therapy and contextual behavioral science: Examining the progress of a distinctive
model of behavioral and cognitive therapy. Behavior Therapy, 44, 180-198.
Hayes, S. C., Luoma, J. B., Bond, F. W., Masuda, A., & Lillis, J. (2006). Acceptance and Commitment
Therapy: Model, processes and outcome. Behaviour Research and Therapy, 44, 1-25.
Hayes, S. C., Pistorello, J., & Levin, M. (2012). Acceptance and Commitment Therapy as a unified model
of behavior change. The Counseling Psychologist, 40, 976-1002.
Hayes, S. C., Villatte, M., Levin, M., & Hildebrandt, M. (2011). Open, aware, and active: Contextual
approaches as an emerging trend in the behavioral and cognitive therapies. Annual Review of
Clinical Psychology, 7, 141-168.
Heffner, M., Greco, L. A., & Eifert, G. H. (2003). Pretend you are a turtle: children's responses to
metaphorical versus literal relaxation instructions. Child & Family Behavior Therapy, 25, 19-33.
Heffner, M., Sperry, J., Eifert, G. H., & Detweiler, M. (2002). Acceptance and commitment therapy in the
treatment of an adolescent female with anorexia nervosa: A case example. Cognitive and
Behavioral Practice, 9, 232-236.
Higgins, J. P. T., & Green, S. (Eds.). (2011). Cochrane Handbook for Systematic Reviews of Interventions
[Version 5.1.0]. Retrieved 25/11/13, from: www.cochrane-handbook.org.
Hopewell, S., McDonald, S., Clarke, M., & Egger, M. (2007). Grey literature in meta-analyses of
randomized trials of health care interventions. Cochrane Database Systematic Reviews, 18. doi:
MR000010
James, A. C., James, G., Cowdrey, F. A., Soler, A., & Choke, A. (2013). Cognitive behavioural therapy
for anxiety disorders in children and adolescents (review). . The Cochrane Library, 6, 1-85.
Kazdin, A. E. (1977). Assessing the clinical or applied importance of behavior change through social
validation. Behavior Modification, 1, 427-452.
Kazdin, A. E. (2007). Mediators and mechanisms of change in psychotherapy research. Annual Review of
Clinical Psychology, 3, 1-27.
Kraemar, H. C., Wilson, G. T., Fairburn, C. G., & Agras, W. S. (2002). Mediators and moderators of
treatment effects in randomized clinical trials. Archives of General Psychiatry, 59, 877-883.
Levin, M. E., & Hayes, S. A. (2009). Is Acceptance and Commitment Therapy superior to established
treatment comparisons? Psychotherapy and Psychosomatics, 78, 380.
Livheim, F., Hayes, L., Ghaderi, A., Magnusdottir, T., Hogfeldt, A., Rowse, J., . . . Tengstrom, A. (2014).
The effectiveness of Acceptance and Commitment Therapy for adolescent mental health:
Swedish and Australian pilot outcomes.
Luborsky, L., Singer, G., & Luborsky, L. (1975). Comparative studies of psychotherapies. Is it true that
"everywon has one and all must have prizes"? Archives of General Psychiatry, 32, 995-1008.
Luciano, C., Ruiz, F. J., Vizcaíno Torres, R. M., Sánchez Martín, V., Gutiérrez Martínez, O., & López, J.
C. (2011). A relational frame analysis of defusion interactions in acceptance and commitment
therapy: A preliminary and quasi-experimental study with at-risk adolescents International
Journal of Psychology and Psychological Therapy, 11, 165-182.
Luoma, J. B., Hayes, S. C., & Walser, R. D. (2007). Learning ACT: An Acceptance and Commitment
therapy Skills-Training Manual for Therapists. Oakland,CA: New Harbinger Publications Inc.
Masuda, A., Cohen, L. L., Wicksell, R. K., Kemani, M. K., & Johnson, A. (2011). A case study:
Acceptance and commitment therapy for pediatric sickle cell disease. Journal of Pediatric
Psychology, 36, 398-408.
McLeod, B. D., & Weisz, J. R. (2004). Using dissertations to examine potential bias in child and
adolescent clinical trials. Journal of Consulting & Clinical Psychology, 72, 235-251.
Metzler, C., Biglan, A., Noell, J.,, Ary, D., & Ochs, L. (2000). A randomized controlled trial of a
behavioural intervention to reduce high−risk sexual behaviour among adolescents in high−risk
sexual behaviour among adolescents in STD clinics. Behavior Therapy, 31, 27-54.
Mulrow, C. D. (1994). Rationale for systematic reviews. British Medical Journal, 309, 597-599.
Munder, T., Brutsch, O., Leonhart, R., Gerger, H., & Barth, J. (2013). Researcher alliance in
psychotherapy outcome research: An overview of reviews. Clinical Psycholgy Review, 33, 501-
511.
Murrell, A., & Scherbarth, A. J. (2006). State of the research and literature address: ACT with children,
adolescents and parents. International Journal of Behavioral Consultation and Therapy, 2, 531-
543.
O'Brien, K., Larson, C., & Murrell, A. (2008). Third−wave behavior therapies for children and
adolescents: progress, challenges and future directions. In L. A. G. S. C. Hayes (Ed.), Acceptance
and mindfulness treatments for children and adolescents. Oakland CA: New Harbinger and
Context Press Publications.
Ost, L. (2008). Efficacy of the third wave of behavioral therapies: A systematic review and meta-analysis.
Behaviour Research and Therapy, 46, 296-321.
Ruiz, F. J. (2012). Acceptance and Commitment Therapy versus traditional Cognitive Behavioural
Therapy: A systematic review and meta-analysis of current empirical evidence. International
Journal of Psychology & Psychological Therapy, 12, 333-357.
Safren, S. A., Heimberg, R. G., Brown, E. J., & Holle, C. (1996). Quality of life in social phobia.
Depression and Anxiety, 4, 126-133.
Seibert, A. E. (2011). The effect of thought acceptance and mindfulness on enhancing self-control
behavior of children with ADHD. Southern Illinois University Carbondale, Unpublished
dissertation.
Swain, J., Hancock, K., Hainsworth, C., & Bowman, J. (2013). Acceptance and Commitment Therapy in
the treatment of anxiety: A systematic review. Clinical Psychology Review, 8, 965-978.
Weisz, J. R., McCarty, C. A., & Valeri, S. M. (2006). Effects of psychotherapy for depression in children
and adolescents: A meta-analysis. Psychological Bulletin, 132, 132-149.
Wicksell, R. K., Dahl, J., Magnusson, B., & Olsson, G. L. (2005). Using Acceptance and Commitment
Therapy in the rehabilitation of an adolescent female with chronic pain: A case example.
Cognitive and Behavioral Practice, 12, 415-423.
Wicksell, R. K., Melin, L., Lekander, M., & Olsson, G. L. (2009). Evaluating the effectiveness of
exposure and acceptance strategies to improve functioning and quality of life in longstanding
pediatric pain – A randomized controlled trial. Pain, 141, 248-257.
Wicksell, R. K., Melin, L., & Olsson, G. L. (2007). Exposure and acceptance in the rehabilitation of
adolescents with idiopathic chronic pain – A pilot study. European Journal of Pain, 11, 267-274.
Wilson, K. G., Bordieri, M., Flynn, M. K., Lucas, N., & Slater, R. (2011). Understanding acceptance and
commitment therapy in context: A history of similarities and differences with other cognitive
behavior therapies. In J. D. Herbert & E. M. Forman (Eds.), Acceptance and Mindfulness in
Cognitive Behavior Therapy: Understanding and applying the new therapies (pp. 233-263).
Hoboken, N. J.: John Wiley & Sons.
Woidneck, M. R., Morrison, K. L., & Twohig, M. P. (2014). Acceptance and Commitment Therapy for
the treatment of posttraumatic stress among adolescents. Behavior Modification, 38, 451-476.
Yardley, J. (2012). Treatment of pediatric obsessive-compulsive disorder: Utilising parent-facilitated
acceptance and commitment therapy. Unpublished doctoral dissertation, Utah State University.
Highlights - 3 to 5 bullet points (maximum 85 characters)
• Systematic review of the evidence for ACT in the treatment of children and adolescents
• Twenty-one studies, including 707 participants, met broad inclusion criteria
• ACT produced improvements in symptoms, quality of life and psychological flexibility
• Methodological caveats were common and larger more stringent studies are warranted
• Preliminary evidence supports the utility of ACT in the treatment of children
Table 1. Overview of included studies by anxiety problem
& %' , '(4
1
($! #'% )
,)
2 3
!"#$% !!%' * .
/ %!
+!,%- # 0 ,5
61
2
78! 9 .!
/ 31% !$
4
8! !)3 . ; ,
:
. 0
< !!%' 9!
", ''% % 4 !
; 7=-
<%:' ! 57 7=-
%'
"( (! ; = 57=
%#'!
/,-!
'+!!%' % / 4 .
(%$
/
08 08
, %1 . ; !" > !" >
9,%
; %
; !( !( 08!" > !(
7!>>!!%'
! %!-% 9 !
37%$!! 4; =
%'
!8! ;/ 0 08!" > !(
4 . 2
3 -,! ! 4 ;4
= ,
%'
; !8! ; 2
#%' % . 0
9!
96!( , / 0
3#" %!
8#' - $) 2 ?-
%'
!
8+'!+!,%- # 0 ?
@%#(%!
%'
9 ":'!"!''( !%! 4 4 9 < 4!
@!*'!! 2 =
. 4 0 ,
%'
9!#%' !(+!,%- # / /
9! +! 4
7 / @ !
0 9
":!''!
%'
%
;
; 9
!
":!''!
./ -
;;", '(
%'
. % ;
. 1;8%!
":!''! %
; . = 0
,
%'
/
", '(5
,
8%!
.
(!": 9!
.
;. ; @
,
; 1
9
.
A%('!$
0 /
2!B+'!> !!B! !> " 7$8!%" - $ (!
7C3!% (!
3C+! -!8#' -! (!
C%#% "!
( (!
9! B%!! !
9!%!9#($
9!6!!#8
=%( !(''!( %'
= , #8
>B!"!% !
>!%'!<%B#+' ,!(% "'!
C08#+' ,!(( !%
08#'% B' "%'
8% !
2"' "%'
2#8% !
0 -! $
0
'"( B%!' !'
@#' 8'!%!' !
@!%!0#%'
0% 3
3!%!B""!8%"!%( !,!%8$
C9!'>'%
9C7%+ =!-!%'%
7=C!( " 8' %$!%!
C?%'#!1!># 8"'
?C?%'#!1
!># 8"'
?<%B<% '$+%!(
<C#8
C( - (#%'
Table 2. POMRF and outcomes for included studies
!
!
+
D=19=
!"9=-!%''9="8#' >!E#!"$D;;4;CA9D444F
. -!
( % G
%-
&
%'
($
! #'
D=", '(!%#!
! %'%- (%"!+!,%- #8+7$81!%"
% +
(!> " C",% ! =&)># !", '(!!">#" 9=%''<0D=
)
; -!
+!,%- #)! #'% ( >> "#' !%!%'&1!#"!% % !(& %'! #'%
!! %-
D! %H-!"8 !'%H-!8!!%!<0=I (>#'!D&)>#
!"#$ %'
*
+!,
%
%-
#
6 !''
1 3 +! D9=&)>#
!%D
.8 = ( "%!(D% !$1(#%H># %H%6!''%I
1
78! 9 ' " %' %
/ % 6
!$ %-
8 !
! ! ' 9=I-%'#!(' - CD&)>#
&)># "!'%!(6 ,%''9"%'!
!"%H%H1
: )3 6 8,+ "% !$
. %-
" !
< !! , '
%' '' 9! 6 D9=>"#!()%#,% 8#''
%+H! 6:( !1 8% !
!'%8!(1!E# !(%
% % %- +!!
!''
" %+
<%:' (
-
!%' (! !
%- D9=H"!-! $
J7=>#"H 1= '+%' 8!
7=K
%#'!
! 9=I%""!8%"!" %')8,$ "%'>#"H (!-!'8!1+L!" -!!%#!CD8% % !$
%
' (!8! "%%8, * C8% ! $!<0
&9J
I9=%""!8%"!
'+! / 6 " %')8,$ "%'>#" +L!" -!!%#!=",'%+!"!=,!%',"%!)!( "% CD9=
%- 8% % !$"%%8, * 8% ! $(!-!'8!1(!8!
!%'
, %
1 !
'
9,% 6
%- D9=1=>#" %'( %+ ' $-! !'''=!%#!K"'%8!%!
; % %(
,=!'% -!8!%,=# !%(%'>#" %'( %+ ' $K'%
% % !(8<0=8,$ "%'( %+ ' $J"'-! !
!
!
7!>>! %
'
6
!%' !- %-
D9=)&#+"%'!M( -!>, !1 !>>!" -!!#+"%'!
"' "%'"' "%'% !&
%
9 +($( % >%" "' "%'% !! ,-!%''I!(C%'% !%<0$8 "%'
!#% !#!(
!''
%+
37%$! !8 =
-
!%' ! !
%- D9=(!8! -!$8
&9J) ;CK0=B-409B4)
!8
! !
'
# 6
4 #%' %#($D9=-!%''(!8! -!$8
&9J($8, %
&9J..%,!( %
%' %-
3 -,! 4
&9J/! % -!!'>!-%'#%
&9J4.% "$8CK0&)>#
%
!%' 96!( ,#($D9=!
&9J CK0&)># 9=N3(!8! !% !$
=
; ; %( !!%'!%',!%',&)># %( (>#'!I%!(%"!"!'%!(6 , 8-!(
9!
+ N3(!8! %(!%
96 -!
!( %-
,
8
#'
- $
) !
?D9=8++!,%- #&)># 1I%""!8%"!%"H!% % !(%<07 , :
3#" % 8 '
D9=",% ! &)># 18I%""!8%"!% % !(%<0?%"!%#!
!%' +'! 6
?K?
%-
+!,
%-
#
9 ":' !''
! +!
@%#(% "!'' . ",% !9=8% 9=" %'% !$1N3 %'% !8!%(8%<0
9
'
!%' ( ! 6 8-!!,!!!%#!I=",'8!>%"!1D&)># %<0I=8%!
%! 9 %- %""!8%"!1D( !-!H!
9!
#%' !'' ,B9=<!E>!M% !>>!"0K
@%'!0K'',!!>>!"
!( %+ 4,B9=2#+!>8%!M% !>>!"K0C@%'!K0
ƉJ>!%'!C&
@!*'! +!, = - , !%'!)>!%'!K09=2 %#M% !>>!"K0C&, !
!%' %- ! %'!)>!%'!K09!6 ,% !CK0@% L#%%#!CK09" %'"8!!"!C
# / %- K0
9! +! 7 ! I=!'>"'
(!'%$>("#8 '!%"! !IB4
C;/.
1C
' .
6
%-
!''
+!
":!' . D9=>#"H%'( %+ ' $%(8% I9=!H>"#!("8
D! %'%- (%"!
'
'!%' 6 @% % !(4,<09=8+'!>"#!(%- (%"! I=",'%O!(%"!19=
% 9 %- -%'#!+%!( %'4,<0
+
":!' -! D9=>#"H%'( %+ ' $
&9J ",'%+!!!
&9J 8% ! $
&9J 8%
'!%' %- !>!!"!
&9J ."%%8,
&9J/=!#'% % !(%(4,<09! $B
. % ; . )/ ).C!>!!"!B4)/ )
+
":!' = . -! I>#"H D !>!!"!1IN3
&9J;.0I>#"H 1D !>!!"!
'!%' %-
&9J N3" !K0>#" %'%+ ' $ ! $1( ">
/ % %%8, * +(!' !
ƉJ 1(!8! >
(! + D9=$8
44/"# $1/ 8% !)4."# $1.; 8% !1
": . 9! 4 -! &)>#
4"# $1. 8% !)4"# $1; 8% !D=$8
.
; 9 %- 8% !14 "# $). 8% !%(4"# $9B8% " 8%,%(98!
F( %
+
A%('!$ D=9=+! >!E1 ! $D% )P-!%''>!E#!"$ /D1 ! $
4 -!
DG
%-
2!B$",,!%8$#"!@!,(' $=% <
@=<+'!> !!B! !> " 7$8!%" - $ (!
7C3!% (!
3C+! -!8#' -! (!
C%#% "!( (!
9! B%!! !
9!%!9#($
9!6!!#8
=%( !(''!( %'
= , #8
#"!BK
!%! 8-!!C""!8%"!%( !,!%8$
C !>9$8
-!$
9C(
C' " %=%!(
=C' "%'=!"-!$
=!"C' "%''$9 > "%,% !
9C&% (!-!$
&C&>>!" *!
&9C
&, " $
&C&8! ! %'%- (%"!
&C<''6#8
<0C!(!
C7%+ =!-!%'%
7=C29 > "%
C% " 8%)
C=!' %+'!,% !
=C9!'>=!8
9=C%!=!8
=C!%!0#%'
0CG2% "%'!"(#"!(
Appendix A. Reasons for exclusion
Study Reasons for exclusion
Asmundson and Hadjistavropolous (2006) Commentary article
Bass, van Nevel, and Swart (2014) Commentary article
Coyne, McHugh, and Martinez (2011) Review article
Gundy, Woidneck, Pratt, Christian, and Review article
Twohig (2011)
Hadlandsmyth, White, Nesin, and Greco Theoretical paper
(2013)
Hannan and Tolin (2005) Theoretical book chapter
Kaiser (2012) Theoretical paper
Murrell and Scherbarth (2006) Review article
Robinson, Gregg, Dahl, and Lundgren No psychometrics measures employed
(2005)
Rowland (2011) Theoretical paper
Ruiz (2010) Review article
Ruiz (2012) Review article
Zehnder, Meuli, and Landolt (2010) Not an ACT intervention
References (Appendix A)
Asmundson, G. J. G., & Hadjistavropolous, H. D. (2006). Acceptance and Commitment Therapy
in the rehabilitation of a girl with chronic idiopathic pain: Are we breaking new ground?
Cognitive and Behavioral Practice, 13, 178-181.
Bass, C., van Nevel, J., & Swart, J. (2014). A comparison between dialectical behavior therapy,
mode deactivation therapy, cognitive behavioral therapy, and acceptance and
commitment therapy in the treatment of adolescents. International Journal of Behavioral
Consultation and Therapy, 9, 4-8.
Coyne, L. W., McHugh, L., & Martinez, E. R. (2011). Acceptance and commitment therapy
(ACT): Advances and applications with children, adolescents, and families. Child and
Adolescent Psychiatric Clinics of North America, 20, 379-399.
Gundy, J. M., Woidneck, M. R., Pratt, K. M., Christian, A. W., & Twohig, M. P. (2011).
Acceptance and Commitment Therapy: State of evidence in the field of health
psychology. The Scientific Review of Mental Health Practice, 8, 23-35.
Hadlandsmyth, K., White, K. S., Nesin, A. E., & Greco, L. A. (2013). Proposing an Acceptance
and Commitment Therapy intervention to promote improved diabetes management in
adolescents: A treatment conceptualization. International Journal of Behavioral
Consultation and Therapy, 7, 12-15.
Hannan, S. E., & Tolin, D. F. (2005). Mindfulness and acceptance based behavior therapy for
obsessive-compulsive disorder. In S. M. Orsillo & L. Roemer (Eds.), Acceptance and
mindfulness-based approaches to anxiety: Conceptualization and treatment (pp. 271-
299). New York: Springer.
Kaiser, D. L. (2012). Mindfulness and acceptance and commitment therapy intervention for
adolescents who have a parent diagnosed with cancer. (Unpublished doctoral
dissertation), Widener University.
Murrell, A., & Scherbarth, A. J. (2006). State of the research and literature address: ACT with
children, adolescents and parents. International Journal of Behavioral Consultation and
Therapy, 2, 531-543.
Robinson, P., Gregg, J., Dahl, J., & Lundgren, T. (2005). ACT in medical settings. In S. C.
Hayes & K. D. Strosahl (Eds.), A Practical Guide to Acceptance and Commitment
Therapy (pp. 295-314). New York: Springer Science & Business Media.
Rowland, M. (2011). Acceptance and commitment therapy for non-suicidal self-injury among
adolescents. (Unpublished doctoral dissertation), The Chicago School of Professional
Psychology.
Ruiz, F. J. (2010). A review of Acceptance and Commitment Therapy (ACT) empirical
evidence: Correlational, experimental psychopathology, component and outcome studies.
International Journal of Psychology and Psychological Therapy, 10, 125-162.
Ruiz, F. J. (2012). Acceptance and Commitment Therapy versus traditional Cognitive
Behavioural Therapy: A systematic review and meta-analysis of current empirical
evidence. International Journal of Psychology & Psychological Therapy, 12, 333-357.
Zehnder, D., Meuli, M., & Landolt, M. A. (2010). Effectiveness of a single-session early
psychological intervention for children after road traffic accidents: A randomised
controlled trial. Child and Adolescent Psychiatry and Mental Health, 4, 1-10.
Records identified Records identified through
through electronic reference lists and citation
databases (n = 169) searches (n = 33)
Records screened on the Records excluded
basis of title and abstract (n = 169)
(n = 202)
Full text articles
Full text articles assessed excluded (for
for eligibility (n = 33) reasons see
Appendix A; n =13)
Articles included in
narrative synthesis (n =20)
You might also like
- Systemic Ethics TextbookFrom EverandSystemic Ethics TextbookKristina S BrownNo ratings yet
- NURS6035 Guide To Assessment 1 Written Assignment 1 Psychosocial Intervention Theory1-1Document12 pagesNURS6035 Guide To Assessment 1 Written Assignment 1 Psychosocial Intervention Theory1-1Zunaira ArshadNo ratings yet
- Cognitive and Behavioral Interventions in the Schools: Integrating Theory and Research into PracticeFrom EverandCognitive and Behavioral Interventions in the Schools: Integrating Theory and Research into PracticeRosemary FlanaganNo ratings yet
- The Six Cycles Maintenance Model Growing A Vicious Flower For DepressionDocument12 pagesThe Six Cycles Maintenance Model Growing A Vicious Flower For DepressionDIANA SPRINCEANUNo ratings yet
- Write Down The History of Abnormal Psychology in Renaissance PeriodDocument12 pagesWrite Down The History of Abnormal Psychology in Renaissance PeriodKashish GautamNo ratings yet
- 2 - Grazebrook, K & Garland, A. (2005) - What Are Cognitive and - Orbehavioural Psychotherapies - Paper Prepared For UKCP - BACP PDFDocument5 pages2 - Grazebrook, K & Garland, A. (2005) - What Are Cognitive and - Orbehavioural Psychotherapies - Paper Prepared For UKCP - BACP PDFAnastasiya PlohihNo ratings yet
- Hospital Project ViabilityDocument12 pagesHospital Project ViabilityMunia Hassan100% (5)
- Ability360's Site: About The DesignDocument36 pagesAbility360's Site: About The DesigndominicjimenezNo ratings yet
- IGNOU Prospectus 2016Document99 pagesIGNOU Prospectus 2016Abhinav MathurNo ratings yet
- Collaborative Problem Solving: An Evidence-Based Approach to Implementation and PracticeFrom EverandCollaborative Problem Solving: An Evidence-Based Approach to Implementation and PracticeAlisha R. PollastriNo ratings yet
- Personality Traits and Anxiety SymptomsDocument19 pagesPersonality Traits and Anxiety SymptomsSusana Díaz100% (1)
- Generalized Anxiety Disorder: Timothy A. Brown Tracy A. O'Leary David H. BarlowDocument55 pagesGeneralized Anxiety Disorder: Timothy A. Brown Tracy A. O'Leary David H. BarlowCamila JoaoNo ratings yet
- MBT-I ManualDocument48 pagesMBT-I ManualLaura AndreiNo ratings yet
- Interpersonal TheoryDocument8 pagesInterpersonal TheoryKenneth ObrienNo ratings yet
- Ipt For Social Anxiety DisorderDocument2 pagesIpt For Social Anxiety DisorderPramita BanikNo ratings yet
- Social Anxiety DisorderDocument6 pagesSocial Anxiety Disordernicole.recedeNo ratings yet
- Dialectical Behavior TherapyDocument5 pagesDialectical Behavior TherapyAhmed AlabwabiNo ratings yet
- 1999 Aversion Therapy-BEDocument6 pages1999 Aversion Therapy-BEprabhaNo ratings yet
- Asma - Report For QOLIDocument5 pagesAsma - Report For QOLIpragati100% (1)
- Guilford Press FlyerDocument2 pagesGuilford Press Flyerskkundor0% (1)
- Wells Brief Cognitive Therapy For Social Phobia - A Case SeriesDocument8 pagesWells Brief Cognitive Therapy For Social Phobia - A Case SeriesjuaromerNo ratings yet
- Adolescent Depression Literature ReviewDocument8 pagesAdolescent Depression Literature ReviewShowbiz ExposeNo ratings yet
- CTSR Cognitive Therapy Rating ScaleDocument15 pagesCTSR Cognitive Therapy Rating Scalechrispalmer21No ratings yet
- Dual Relationships Between TherapistDocument18 pagesDual Relationships Between TherapistVictor Hugo Esquivel100% (1)
- Understanding Schizophrenia: Helping Families & Friends Find Better WaysDocument4 pagesUnderstanding Schizophrenia: Helping Families & Friends Find Better WaysSee EssNo ratings yet
- What? Me Worry!?! What? Me Worry!?!Document7 pagesWhat? Me Worry!?! What? Me Worry!?!KonkmanNo ratings yet
- Other Cognitive Behaviour TherapiesDocument13 pagesOther Cognitive Behaviour TherapiesJasroop Mahal100% (1)
- Exposure and Response PreventionDocument6 pagesExposure and Response PreventionshobaNo ratings yet
- Child Is A Discouraged Child," and That Children's Behavior Patterns Improve MostDocument7 pagesChild Is A Discouraged Child," and That Children's Behavior Patterns Improve MostMaleeka PrettyNo ratings yet
- Patterson Cognitive Behavioral Systems ApproachDocument14 pagesPatterson Cognitive Behavioral Systems ApproachSusana FossaNo ratings yet
- CH 5 Psychointetherap 2Document17 pagesCH 5 Psychointetherap 2Elif AktaşNo ratings yet
- Patient-Centered Care at The End of Life.07Document52 pagesPatient-Centered Care at The End of Life.07api-3755169100% (1)
- What Is Psychotherapy - OdtDocument3 pagesWhat Is Psychotherapy - Odtsehar arif100% (1)
- Sample Case Study For DMS-IV-TRDocument6 pagesSample Case Study For DMS-IV-TRohphooeyNo ratings yet
- GAD General Anxiety DisorderDocument9 pagesGAD General Anxiety Disorderselina shakyaNo ratings yet
- Tejares, de Guzman, CapunoDocument43 pagesTejares, de Guzman, CapunoKyra Jane F. DellosaNo ratings yet
- Child DisordersDocument111 pagesChild Disorderspriyanka raj100% (1)
- Brief Strategic Family TherapyDocument13 pagesBrief Strategic Family TherapyJoana CarvalhoNo ratings yet
- SchizophreniaDocument9 pagesSchizophreniavinodksahuNo ratings yet
- Castonguay+et+al+ 1996Document8 pagesCastonguay+et+al+ 1996Pamela Cortés PeñaNo ratings yet
- PTSDDocument17 pagesPTSDadrianaNo ratings yet
- Bipolar QRGDocument24 pagesBipolar QRGRe LzNo ratings yet
- Research Methods - Final Research ProposalDocument10 pagesResearch Methods - Final Research Proposalapi-583124304No ratings yet
- CBT Competences - Map Sept 2015Document1 pageCBT Competences - Map Sept 2015Roxana BlejeruNo ratings yet
- Case Presentation and Treatment ArchivesDocument3 pagesCase Presentation and Treatment ArchivesДоника100% (1)
- Lesson 2 The Skills Activities of A Clinical PsychologistDocument6 pagesLesson 2 The Skills Activities of A Clinical Psychologistjericho anchetaNo ratings yet
- FT and Systemic PracticeDocument4 pagesFT and Systemic PracticeAndra AndruNo ratings yet
- Understanding Anxiety in Children and Teens: 2018 Children's Mental Health ReportDocument20 pagesUnderstanding Anxiety in Children and Teens: 2018 Children's Mental Health ReportBernard Sid AhmedNo ratings yet
- NSW Department of Health 2004 Suicide Risk Assessment and Management Protocols General Community Health ServiceDocument20 pagesNSW Department of Health 2004 Suicide Risk Assessment and Management Protocols General Community Health ServiceLuna MArinaNo ratings yet
- Psychodiagnostics and Psychological AssessmentDocument4 pagesPsychodiagnostics and Psychological AssessmentBim arra0% (1)
- Theraputic Intervention. Uzair AhmedDocument4 pagesTheraputic Intervention. Uzair AhmedUzair RiazNo ratings yet
- Avoiding Burnout and Severe Stress: Guidelines For The Helping ProfessionalsDocument44 pagesAvoiding Burnout and Severe Stress: Guidelines For The Helping ProfessionalsChiriac Ionut IlieNo ratings yet
- PTSD EXAMDocument53 pagesPTSD EXAMJohnny JoeNo ratings yet
- Tratamentul DeliruluiDocument14 pagesTratamentul DeliruluiSendruc OvidiuNo ratings yet
- Understanding When Psychotherapy Is A Controlled ActDocument3 pagesUnderstanding When Psychotherapy Is A Controlled Actbobbie carefoote100% (1)
- S6 Emotion Regulation StrategiesDocument4 pagesS6 Emotion Regulation StrategiesRăzvan-Andrei ZaicaNo ratings yet
- PSYCH - PsychosomaticdelasalleDocument58 pagesPSYCH - Psychosomaticdelasalleapi-3856051100% (1)
- Cognitive Behavioral Model of Obsessive Compulsive Disorder Salkovskis Forrester Richards 1998 Lang Eng Us Format ProfessionalDocument6 pagesCognitive Behavioral Model of Obsessive Compulsive Disorder Salkovskis Forrester Richards 1998 Lang Eng Us Format ProfessionalSara NevesNo ratings yet
- Shalit - Efficiency of PsychotherapyDocument9 pagesShalit - Efficiency of PsychotherapyAyerevNo ratings yet
- Coun523 Final Paper Treatment PlanDocument11 pagesCoun523 Final Paper Treatment Planapi-717187506No ratings yet
- Play Therapy MenassaDocument15 pagesPlay Therapy MenassaNur Hidayah DaniNo ratings yet
- Psychological Formulation and Treatment PlanDocument26 pagesPsychological Formulation and Treatment Planzwidofhela363No ratings yet
- Martha RogerDocument2 pagesMartha RogerAlyssa Mae AzarconNo ratings yet
- 2.1 Physical SelfDocument80 pages2.1 Physical SelfZharianne GerminalNo ratings yet
- PSP RepairDocument41 pagesPSP RepairKelvin LauNo ratings yet
- Manual HandlingDocument37 pagesManual HandlingSherylyn BanaciaNo ratings yet
- Ecologies of Suffering: Mental Health in IndiaDocument4 pagesEcologies of Suffering: Mental Health in Indiakimice5490No ratings yet
- CSAHCA0042A Attend to Sanitation and Hygiene CareDocument65 pagesCSAHCA0042A Attend to Sanitation and Hygiene Caretash.shanebowmanNo ratings yet
- Abstracts From The 5th International PDFDocument201 pagesAbstracts From The 5th International PDFMohamed Ben RejebNo ratings yet
- Firex MSDS Be 020518Document8 pagesFirex MSDS Be 020518Eng.Ibrahim OthmanNo ratings yet
- II. IDENTIFICATION: Identify What Is Being Described in Each Number. Choose The Answer at The BoxDocument4 pagesII. IDENTIFICATION: Identify What Is Being Described in Each Number. Choose The Answer at The BoxAthena JozaNo ratings yet
- (Urinary System, Digestive System and Nervous System) : My Lost HopesDocument3 pages(Urinary System, Digestive System and Nervous System) : My Lost HopesCesar Dave PresentacionNo ratings yet
- Recommended Devices For TCCCDocument1 pageRecommended Devices For TCCCGiovanni Rana100% (1)
- English File 3e - Upper-Int SB-strony-15-18,135,160Document6 pagesEnglish File 3e - Upper-Int SB-strony-15-18,135,160MarioNo ratings yet
- Good Maintenance Performance: SDN BHDDocument10 pagesGood Maintenance Performance: SDN BHDEng. Ahmed MuneerNo ratings yet
- Mini Pupillage Cover Letter SampleDocument5 pagesMini Pupillage Cover Letter Sampleuifujzhfg100% (2)
- DONE Healthy Married Sex LifeDocument2 pagesDONE Healthy Married Sex LifeRxAdamNo ratings yet
- Top Messages: Paediatric Life Support 2021Document6 pagesTop Messages: Paediatric Life Support 2021Mihai Ion GhioaldaNo ratings yet
- Level 3 Self Assessment Specialization in Infectious Disease NursingDocument21 pagesLevel 3 Self Assessment Specialization in Infectious Disease Nursingmacbookairgumabay25No ratings yet
- SF 9 - ES ( (Learner's Progress Report Card)Document2 pagesSF 9 - ES ( (Learner's Progress Report Card)Willyn Grace Mollanida Buban100% (7)
- The Ergonomic Solution To Backbreaking Tasks: 5-Minute Safety Talk by Osha ProsDocument2 pagesThe Ergonomic Solution To Backbreaking Tasks: 5-Minute Safety Talk by Osha ProsWelma JohnsonNo ratings yet
- Hse Indian StdsDocument11 pagesHse Indian StdsSatya NaiduNo ratings yet
- Full Download Brenner & Rector's The Kidney 11th Edition Alan S. L. Yu PDFDocument64 pagesFull Download Brenner & Rector's The Kidney 11th Edition Alan S. L. Yu PDFsuyasaoce100% (4)
- ADIL BSN - 1C 11. Manual Reproductive SystemDocument4 pagesADIL BSN - 1C 11. Manual Reproductive SystemReiko SakaeNo ratings yet
- A Cost Analysis of Labour Party Policy For 2015-2016Document86 pagesA Cost Analysis of Labour Party Policy For 2015-2016Harry ColeNo ratings yet
- Data SheetsDocument90 pagesData Sheetswilson chinyamurindiNo ratings yet
- Investigative Field Essay Project 1Document12 pagesInvestigative Field Essay Project 1api-744284701No ratings yet
- ZVP PC 0072 01 PDFDocument6 pagesZVP PC 0072 01 PDFvijay moriNo ratings yet
- أثر استخدام تكنولوجيا المعلومات و الاتصال على تحسين الأداء الوظيفي للعاملين في مكاتب المحاسبة خلال أزمة فيروس كورونا - كوفيد19- (دراسة تطبيقية على عينة من مكاتب المحاسبة في الجنوب الشرقي)Document14 pagesأثر استخدام تكنولوجيا المعلومات و الاتصال على تحسين الأداء الوظيفي للعاملين في مكاتب المحاسبة خلال أزمة فيروس كورونا - كوفيد19- (دراسة تطبيقية على عينة من مكاتب المحاسبة في الجنوب الشرقي)salm yasmenNo ratings yet