
CT Sim Commissioning Process
Uploaded by
Eskadmas BelayCT Sim Commissioning Process
Uploaded by
Eskadmas BelaySee discussions, stats, and author profiles for this publication at: https://www.researchgate.
net/publication/231905294
Commissioning a new CT simulator I: CT simulator hardware
Article in Journal of Radiotherapy in Practice · September 2007
DOI: 10.1017/S1460396907006097
CITATIONS READS
4 2,132
2 authors:
Denise Irvine Mark Mcjury
Belfast Health and Social Care Trust University of Glasgow
26 PUBLICATIONS 121 CITATIONS 54 PUBLICATIONS 1,324 CITATIONS
SEE PROFILE SEE PROFILE
All content following this page was uploaded by Mark Mcjury on 16 March 2018.
The user has requested enhancement of the downloaded file.
Journal of
Journal of Radiotherapy in Practice (2007)
Radiotherapy 6, 153 162
2007 Cambridge University Press
in Practice doi: 10.1017/S1460396907006097
Original Article
Commissioning a new CT simulator I: CT simulator hardware
D. Kearns, M. McJury
Department of Medical Physics, Northern Ireland Cancer Centre, Belfast, N. Ireland
Abstract
This paper reports on the commissioning tests performed on a new GE Lightspeed RT wide-bore computed
tomography (CT) scanner with GE Advantage Sim software. This paper focuses on the laser marking sys-
tem, CT hardware and the interfaces between each component of the system, and generalises the findings
to most CT simulation systems currently available. A discussion on the commissioning of the virtual
simulator software will follow in a separate paper. Three phantoms were used (two constructed in-house)
to assist with a range of tests covering aspects such as the laser patient marking system, CT hardware,
and connections between the CT scanner, virtual simulator system and the treatment planning system
(TPS) and VARiS. Tests performed showed the CT simulation system to be working within acceptable
tolerances suggested in the literature, and baseline data have been obtained against which future
comparisons of system performance have been made. Where no tolerances were available, we have sug-
gested suitable values. While considering tolerances on Hounsfield number variation that may lead to a
dose error in excess of 2%, we found that in the case of low-kV CT scanning the range of Hounsfield
numbers for dense bone was outside the acceptable limits for potential dose errors and so users were
advised not to perform radiotherapy planning CT scans with kV below 100 kV.
Keywords
Commissioning; CT simulation system; quality assurance
INTRODUCTION patient for verification, it offers the possibility to
miss out a patient visit for physical verifica-
Simulation continues to be an important part of tion. The CT simulator consists of a diagnostic
the radiotherapy process for acquiring localisa- quality CT scanner with a flat patient couch, a
tion data and treatment verification. Computed computer-controlled moveable laser marking
tomography (CT) simulation1 is being increas- system and a virtual simulator (VS) workstation.
ingly implemented in this process to replace the
simulation on a conventional simulator as it offers The acceptance testing and commissioning
significant advantages:2 (1) it offers the ability to procedures carried out on a new CT simulator
acquire a complete volume data set; (2) it enables should evaluate each component of the system
the generation of sophisticated digitally recon- thoroughly in order to assess whether or not it
structed radiographs (DRRs) for treatment portal meets with the specifications and acceptable tol-
verification; (3) having the data for the virtual erances, and to obtain baseline values against
which future quality assurance (QA) of the sys-
tems can be measured. Currently, there is a
Correspondence to: D. Kearns, Department of Medical Physics,
Northern Ireland Cancer Centre, Belfast City Hospital, Lisburn Road,
dearth of information available on commission-
Belfast BT9 7AB, N. Ireland. E-mail: denise.kearns @mpa.n-i.nhs.uk ing CT simulators;3 6 therefore this report aims
153
Commissioning a new CT simulator I: CT simulator hardware
to set out the commissioning that was per- available QA tools and phantoms. Commission-
formed on the new CT simulation system (GE ing and routine QA of a CT simulator consists
Lightspeed RT wide-bore CT scanner with GE of a significant range of tests, and most probably
Advantage Sim software v6) installed at the more than one phantom will be required to
Northern Ireland Cancer Centre, and generalise perform the all tests. When broken down into
that discussion to apply the guidelines applic- groups of similar tests, a few fairly simple phan-
able to most systems currently available. This toms are all that will be required and these
paper concentrates on the laser marking system, could be constructed easily by an in-house
CT hardware and the interface between each mechanical workshop. A range of commercial
component of the virtual simulation system. phantoms are also available.7,8 A commercial
A discussion on the virtual simulation software, phantom, in particular, may be preferred for
including DRR generation and multimodality the assessment of Hounsfield number (HN) and
image registration, will follow in a separate electron density accuracy of the CT simulator,
paper. for example, the QUASAR phantom (SeeDOS
Ltd.) and the CIRS phantom (Imaging Equip-
ment Ltd./Southern Scientific). We have built
METHODS a range of phantoms in-house for commission-
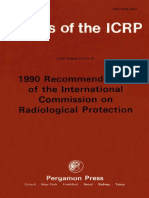
Commissioning tests can be sub-divided along ing and routine QA. Figure 1 shows the laser
functional lines for the system. The CT simula- check phantom, loosely based on a phantom
tor involves an integration of several systems available from Nuclear Associates. The phan-
and so it is crucial that not only the individual tom consists of a flat base-plate with a central
systems themselves are tested but also the trans- 1-mm diameter ball-bearing. Twin pairs of
fer of data between them (particularly coordi- crossed wires are positioned 10 cm each side
nates) is tested for accuracy and robustness. of the centre, along the same axis. Marks are
etched on the sides of the phantom, enabling it
to be positioned in alignment with lateral lasers,
Phantoms and a spirit level on top enables the phantom to
The tests a user performs will depend not only be levelled. This is useful as the flat-top couch
on the equipment specification but also on the insert may be removed, for example, to perform
(a) Alignment
Ball bearing markings
Wires
Levelling feet
(b)
(c)
Figure 1. Laser check phantom and acquired 1.25 mm slice thickness CT images. (a) shows a schematic diagram of the phantom;
(b) shows the central image when the phantom is aligned with lateral lasers offset in the Sup Inf direction. When the phantom is
aligned with lasers that have been correctly positioned, the three markers line up on the central slice, (c).
154
Commissioning a new CT simulator I: CT simulator hardware
a test on CT number uniformity with the CT and a centre line etched on the anterior face assist
manufacturer’s QA phantom; and, in this case, with alignment with the lasers.
although there are fixation screws at the end to
lock it in position when it is replaced, there can
still be a slight movement in the couch when it Laser marking system
is ‘locked’. Daily checks by radiographers on the In terms of the order of performing tests, it is use-
unit can be done quickly and easily with a cube ful firstly to ensure the laser marking system is
phantom (which assumes the couch to be level). correct and use this as a tool to check the CT
This is a hollow plastic cube, typically 15 cm couch geometry and movement. The laser system
along its sides, with etched marks to align the in situ may vary depending on the needs of a
phantom with the sagittal and lateral lasers, and particular department, but, in general, available
1-mm ball-bearings positioned centrally on lat- systems mainly vary in terms of the degree of
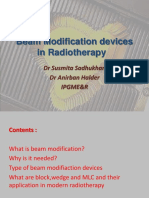
eral and anterior faces. We also have a simple motion of the lasers. Irrespective of the particular
Perspex and wire cube phantom to test the CT system installed, the same general set of tests is
Sim and treatment planning process (Figure 2). applicable for commissioning the laser marking
This solid cube phantom (15 cm along each system. In our department, a Dorado-3 system
side) has a set of embedded wires that reprodu- (L.A.P. lasers, Germany) was installed, consisting
cibly define a PTV of known size and volume. of two wall-mounted lateral lasers (with fixed
Two ball-bearings positioned on the lateral faces vertical and moveable horizontal laser compo-
nents) and a ceiling mounted tracking sagittal
laser. A summary of the tests carried out on the
laser marking system described in detail below
15 cm can be found in Table 1.
7 cm
The laser orientations in the horizontal and
vertical must be tested to ensure they are true.
For the vertical, this can be easily performed
using a conventional plumb-line at commis-
10 cm
sioning and checked during routine QA by
15 cm
standing a long precision level vertically and
5 cm ensuring the laser follows the edge of the level.
A self-levelling laser-projection level (e.g. Fisco
multi-point self-levelling 5-point laser, Fisco
10 cm
Tools Ltd, Essex, U.K.) is very useful in setting
up the horizontal lateral lasers truly level. It can
also be twisted out of plane of the lateral lasers
to allow the horizontal lasers to be checked for
trueness ‘along the couch’. The lateral lasers
must be coincident with each other in the ver-
tical and horizontal orientations. This is easily
checked using a small piece of film. Coincid-
ence is especially important within a maxi-
mum patient volume positioned on the couch
(within approximately 50 cm of isocentre in
all three orthogonal directions). In the case of
our Dorado-3 system, the overhead unit also
projects a fixed lateral beam, which is coin-
cident with the vertical beams from the lateral
Figure 2. Schematic and central CT image of the Perspex and laser pair. This is somewhat surplus to the
wire cube phantom showing the six wire markers and the two requirement, and may be turned off/blocked
ball-bearings on either side of the phantom. as it adds a further laser to be routinely checked
155
Commissioning a new CT simulator I: CT simulator hardware
Table 1. Summary of tests carried out on the laser marking system
System Function Test Suggested tolerance Results
Laser marking Reference mark Laser setup accuracy All laser positions accurate Moveable laser positioning
system marking to within 1.0 mm3 accurate to <0.5 mm
Angular divergence over a range –50 cm
<1 over 100 cm3 from isocentre
Laser offset from gantry
accurate to 1.0 mm
Co-ordinate transfer from Error 1.0 mm at maximum Deviation <1.0 mm from
virtual simulator positions3 planned position
in all axes
and adjusted without adding any real value to position to be fine-adjusted by the user. This
the system setup. The sagittal laser should be provides ease of patient access for tattooing the
coincident with the centre of the X-ray beam laser marks.
and, in turn, the patient couch should track
the sagittal laser. Unlike a linac, where a base- First, the absolute offset should be checked.
frame system is used to ensure the patient couch A phantom or opaque marker can be aligned
and gantry are accurately perpendicular to each with the lateral lasers, moved 500 mm into the
other, this design tends not to be the case for gantry, and imaged to confirm (this assumes
CT systems, even those for exclusive radio- the calibration of couch longitudinal movement
therapy use. At commissioning, therefore, it is to have been checked previously). This avoids
important to ensure that the couch is centred errors where the lateral lasers may be coin-
to the X-ray fan beam, and motion is found to cident, but angled to point towards or away
be perpendicular to the X-ray beam. An X-ray from the gantry (in/out of axial plane). Second,
opaque marker may be placed on the patient two markers may be placed on the patient
couch to mark the position of the sagittal laser. couch at a large distance on either side of the
The marker should be 1 mm diameter to sagittal laser, in line with the lateral lasers, and
ensure the lasers meet a tolerance for accuracy set the marker position as the isocentre slice
of –1 mm. When imaged, any offset of the laser position (most scanners allow any z-position to
from X-ray isocentre (the centre of an image) be set as ‘zero’ or centre of the scan volume).
can easily be obtained from the co-ordinates of With the acquisition of a set of thin (ideally
the marker, either read directly from the CT 1-mm thickness or less) axial slices, the position
image or after the images have been transferred of the markers will verify the offset of the lasers
to the VS and corrected. The marker can be to gantry centre. In addition, if both lasers are
moved down the patient couch, and a series of at the same offset distance, both markers should
CT topograms quickly confirm the tracking of appear with equal distinctness in each axial
the couch with the laser. image. If this is not the case and one is out of
alignment with the other along the z-direction,
The moveable lasers should display linearity this indicates that the lasers are at an angle to the
of movement. This can be easily verified with CT gantry. By placing another marker in line
a metre rule on the patient couch or using a with the other two markers, but at the X-ray
metal tape measure placed and secured vertically beam centre, an image showing equal distinct-
for the lateral lasers. The installed LAP lasers ness for all three markers will ensure that the
performed with <0.5 mm deviations over a lateral lasers are truly running parallel to the
measured range of –50 cm from isocentre. X-ray fan beam and not orientated in or out
of the plane of the image (i.e. verification that
The lateral lasers will generally be installed at the lasers are truly parallel to the X-ray fan
a known distance from the front of the gantry beam and that the offset is accurate to within
(typically 500 mm), allowing the final laser –1 mm).
156
Commissioning a new CT simulator I: CT simulator hardware
The horizontal plane of the lateral lasers should IMPACT website: www.impactscan.org and in
coincide with the isocentre of the X-ray beam. the IPEM Report 91.9
This may be checked most easily using the two
markers on the patient couch described earlier. The CT couch should perform in the same
Position the patient couch such that the markers manner as a treatment couch, in terms of
accuracy and precision of movement and deflec-
are aligned with the lateral lasers. On an acquired
image, their horizontal coordinate should be the tion (sag). At commissioning, the couch move-
same (this may be verified from the pixel coordi- ment (loaded with weights simulating a typical
nates or by overlaying a grid on the image). If adult patient) should be checked in the horizontal
and vertical directions. In particular, it is import-
this is not so, although the lasers may be coincid-
ent, they may be directed at an angle clockwise ant to be aware of the differences in couch
or counter-clockwise to true horizontal or the design. The linear accelerator treatment couch
patient couch may not be flat. This can most design (often a so-called scissors type) and CT
easily be investigated and corrected using a laserpatient couch may differ, with some manufac-
projecting level. turers (as in our case with a GE Lightspeed RT
scanner) using a cantilever design for CT couch.
It is possible on some systems to transfer the This may result in differences in performance.
coordinates of the isocentre (or other reference Our checks on couch vertical motion were per-
point) from the VS to the laser system, which formed by attaching a marker to the couch and
will cause the lasers to move to be aligned assessing the change in height indicated by the
with this point. The function will be mentioned marker against the digital display over its full
explicitly later. range of travel. The vertical accuracy and preci-
sion was found to be better than –0.5 mm for
vertical travel. Our GE Lightspeed RT CT
CT hardware couch with the cantilever design also means that
A summary of CT hardware commissioning any vertical movement will also include a hori-
tests can be found in Table 2. zontal movement. The system is engineered
such that, with the gantry lasers on, the couch
The commissioning of the CT scanner in attempts to automatically correct any horizontal
terms of image quality, dosimetry and radiation movement during vertical motion, to ensure the
protection generally falls within the remit of a couch keeps to the same horizontal landmark
Radiation Protection Advisor (RPA), and so is during vertical motion. We found horizontal
beyond the scope of this report. Details on this deviation during vertical movement to be
part of commissioning may be found on the 0.5 mm (gantry lasers on). In the horizontal
Table 2. Summary of CT hardware tests
System Function Test Suggested tolerance Results
CT scanner Image Dosimetry –20% of manufacturer
acquisition specifications4
Image quality Consistent with manufacturer
specifications and
commissioning results4
HN accuracy and the effect Water: baseline –5 HU4 Water: 4.3 – 6.0 HU
of reconstruction kernels
Accuracy and precision of –1.0 mm over typical <1.0 mm for typical
couch motion under load scan range4 patient scan
Table sag should be <4.0 mm over
comparable to a medical full extension
linear accelerator4
157
Commissioning a new CT simulator I: CT simulator hardware
direction, a tape measure was attached to the Table 3. Acquisition protocols
couch and movement against digital display was
Scan Scan kV mA Kernel Slice
assessed against a stationary marker. Again, hori- mode thickness
zontal deviation was better than –0.5 mm. If
the couch is not perfectly level in the superior 1 Axial 120 80 Std 5 mm (1 image
inferior direction, it is possible that as the couch per rotation,
4 · 1.25 mm
extends there will be a difference in height detectors)
between the superior and inferior ends. Setting 2 Axial 120 200 Std 5 mm
up a projection laser level on a platform, such 3 Axial 120 400 Std 5 mm
that it projects along the surface of the couch, 4 Axial 80 100 Std 5 mm
checks how level the couch is, and extending 5 Axial 140 100 Std 5 mm
the couch enables measurement of the deviation a Lung
of the couch surface from the laser at the b Bone
extremes of couch travel. We found the deviation c Detail
from true horizontal to be less than 0.5 mm over d Edge
e Soft
the full range of horizontal couch travel.
6 Helical 120 100 Std 5 mm
(pitch 0.75:1)
At commissioning, it is important to verify 7 Helical 120 100 Std 5 mm
that, in terms of sag under load, the CT patient (pitch 1.5:1)
couch will be performing in a similar way to
the treatment couch. Further, it is important
that there is minimal sag as the couch moves that mimic the HNs of the most common tissue
500 mm from alignment with the external lasers, types. The scanner will generally be calibrated
into the centre of the gantry. Most manufacturers with reference to air and water, so these represent
have a specific procedure to measure couch sag, a minimum for acquired data, although data
which will depend on the couch model (often for a bone insert are also valuable. A series of
involving the setup of a simple dial gauge under scans using typical clinical parameters should
the superior couch end at maximum extension) be acquired to measure the HNs. The scan data
and this should be followed and the results com- should be transferred to the TPS and the cor-
pared to data from sag of the treatment couch. responding electron densities measured. In order
to obtain baseline values for CT numbers and
We loaded the couch with an evenly distrib- determine tolerances, a CT phantom (CIRS
uted 80-kg total load to model a typical patient. Model 062 Electron Density Phantom) contain-
A marker was placed on the couch top and the ing 17 different tissue equivalent inserts was
couch height adjusted to align the marker and scanned a number of times using the acquisition
lateral horizontal laser. The couch was moved protocols as listed in Table 3. The protocols cov-
500 mm into the gantry and the offset from the ered a range of available values for mA, kV and
marker recorded: this was found to be <1 mm. reconstruction kernels. Acquisition protocols 6
Similarly, over full extension, sag was found to and 7 are considered to be the clinical standard
be <4 mm. or default protocol in our department; therefore,
the CT numbers obtained using these protocols
For radical treatments, image data from the CT are considered the baseline for comparisons.
are often used for dose calculation in the treat-
ment planning system (TPS). The TPS will take An important consideration is the tolerance on
the HNs and convert them to electron densities HN/electron density variation, which may lead
for dose calculation, and so it is important to to a dose error in excess of 2%. Using a metho-
measure the HNs and confirm the correct calib- dology described in Kilby et al.,10 for a 6 MV
ration of the scanner. The HNs will depend linac photon beam irradiating a depth of 20 cm
mainly on X-ray tube kV, mA and image recon- of water, 10 cm of lung or 7 cm of bone, a 2%
struction kernel. Several phantoms are commer- error in dose is produced with a change of elec-
cially available, containing a number of inserts tron density of –0.03 for water, –0.05 for lung
158
Commissioning a new CT simulator I: CT simulator hardware
and –0.08 for bone (Table 4). Advantage Sim For the GE Lightspeed CT scanner, the scan
does not give the user electron density informa- field of view (SFOV) is 50 cm and corresponds
tion, so data were transferred to our TPS. The to a maximum display field of view (DFOV).
TPS uses the relations detailed in Knoos et al.11 Using the ‘WideView’ option allows the CT
to determine electron densities based on HNs, image to be reconstructed with a DFOV of
and this formalism was used to generate electron 65 cm. In order to obtain a qualitative assess-
densities and help define tolerances. Our results ment of the efficacy of this algorithm, our
(see Table 5) showed that the range of HNs for Perspex and wire phantom was scanned at the
dense bone was out of the acceptable limits for edges of the SFOV and the ‘WideView’ option
potential dose errors. HN variation is generally used to reconstruct images with a DFOV of
greatest for bone, and for low-kV CT scanning. 65 cm. These images were assessed as being
Our low-kV scan produced an unacceptably geometrically correct.
high HN for bone, and so we advised the users
not to perform radiotherapy planning CT scans
with kV below 100. Data transfer
CT simulation is only one step in the larger
If post-processing filters are used, which affect treatment process. Data will be flowing through
the HNs (on Siemens CT scanners, for example), the CT simulator, and therefore the speed and
these should be included. robustness of data transfer must be assessed.
Archiving is the simplest data transfer protocol,
but arguably one of the most important. On
Table 4. Hounsfield numbers and electron densities for water, lung and
dense bone most VS systems, archiving can be done both
locally onto recordable media (CD-R, DVD,
HN Electron density Tolerance (–) MOD and exabyte tape). It is a simple matter
(·1023 electrons/cm3)
to send some studies to and back from archive,
Water 4.3 3.31 0.03 and check for data integrity via standard check-
Lung (inhale) 820 0.55 0.05 sum methods. Speed of transfer can be assessed
Dense bone 960 4.82 0.08 qualitatively in this situation.
Table 5. Hounsfield numbers and electron densities with varying kV Interface between the CT scanner
for dense bone and the VS
Once the patient CT data have been acquired,
Scan kV mA HN Electron
density the data are transferred to the VS. This link
must be tested to ensure the integrity of the data
1 80 100 1320 5.26 transfer (Table 6). A test phantom (geometric or
2 120 100 960 4.82 anatomical) should be scanned in all clinical
3 140 100 895 4.74
patient orientations and the images transferred
Table 6. Summary of tests on the CT scanner-virtual simulator interface
System Function Test Suggested tolerance Results
CT scanner-virtual Image and Transfer accuracy Successful transfer Successful transfer
simulator interface co-ordinate of all CT data3 of all CT data
transfer Correct transfer of
patient orientation
Transfer speed Speeds within tolerances Data transfer speeds
and robustness set at commissioning satisfactory
for all times of day3
159
Commissioning a new CT simulator I: CT simulator hardware
Table 7. Summary of tests carried out on the virtual simulator—database interface
System Function Test Suggested tolerance Results
Virtual Transfer of images, Accuracy of Accurate transfer of all data Successful
simulator structures and plans data transfer Speeds within tolerances set transfer of all
database to the radiotherapy Speed of data at commissioning for images,
interface database (e.g. VARiS) transfer all times of day1 structures and
plans to VARiS
to the VS to ensure the transferred images are Interface between the VS and the
displayed with the correct orientation. A qualit-TPS/PACS/record and verify systems
ative assessment of transfer may also be made to Once structures/plans/DRRs have been gener-
ensure the network is performing as expected. ated using virtual simulation, the data will gen-
To test the CT-VS interface, our Perspex and erally be sent to a TPS (for dose calculation), or
wire phantom containing a number of wire mar- directly to the department record and verify sys-
kers that could be used for the purposes of repro-
tem (such as VARiS) for conventional veri-
ducible contouring (see Figure 2) was scanned fication or treatment, via a network. As above,
in four different patient orientations (head-first,
transfer tests should be done on the data to
supine; feet-first, supine; head first, prone; and
ensure accuracy and robustness of transfer
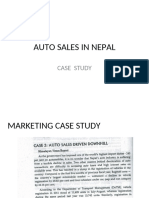
feet-first, prone) and the images transferred to (Table 7). Figure 3a and b shows examples of
the VS. The images were checked for correct CT scans transferred from VS to TPS, where
orientation. The system was found to be robust. the CT orientation was misinterpreted result-
ing in its display as differing to the overlaying
structure contour. Figure 3c shows an example
Interface between the VS and where two different test contours were drawn
the laser marking system manually. When transferred from the VS to
During the planning process on the Advantage the TPS all contours imported onto 1 CT slice.
Sim VS, a ‘marking’ file is created and can be Depending on workflow, some departments
exported and retrieved by a compliant laser may additionally return the plan data to the
marking system, which then moves the lasers VS system for verification and generation of
to the specified coordinates ready for patient geometric setup shifts and DRRs of higher
setup checks. The origin of the coordinate sys- quality than their TPS. In this situation, the
tem used by Advantage Sim is defined as the robustness of data transfer is important in terms
point of intersection of the CT gantry axis and not only of bit-wise integrity of the data but
the scanning plane when the table is in the also of accuracy of parameters and coordinates.
zero offset position. All co-ordinates used and Specifically, when data are moving between
displayed by Advantage Sim are defined relative systems, it is important that the geometry
to this point. The co-ordinate system is refer- and scales (i.e. IEC/non-IEC scales for machine
enced to the centres of the voxels. A scan of movement, patient orientations, MLC leaf
the Perspex and wire phantom was acquired labelling and so on) are not confused at any
and transferred to the VS. An off-centre isocen- point. It is useful to acquire a set of phantom
tre was defined at a known geometric position, scans in the four typical patient orientations,
and the coordinates of the reference laser posi- generate a plan on these data sets and transfer
tions were exported to the LAP laser system. them through the anticipated work-flow for
The couch was moved to the landmarked zero the departmental treatment. A set of standard
position, and the lasers were then automat- plans can be generated and used for routine
ically driven to the newly defined isocentre QA in a similar fashion. The process described
position. Deviation from planned isocentre in the previous section for checking transfer of
was <1 mm in all axes. orientation was further extended to include
160
Commissioning a new CT simulator I: CT simulator hardware
Lightspeed RT wide-bore CT scanner with
GE Advantage Sim software) installed at the
Northern Ireland Cancer Centre. We have
attempted to generalise the discussions to be
applicable to the performance on most CT
simulation systems currently available.
Phantoms required for initial commissioning
(a) and subsequent quality control tests, both avail-
able commercially and constructed in-house,
have been described.
Tests carried out on the laser marking system,
the CT scanner hardware and the interfaces bet-
ween the CT scanner and the VS and between
the VS and the laser marking system/TPS/
PACS/Record and Verify systems have been
(b)
described. The system was generally found to
be working within suggested tolerances obtained
from literature currently available, and where
there are no tolerances available, we have sug-
gested suitable values. However, while determin-
ing tolerances for HNs, by considering the
variation that may lead to a dose error in excess
of 2%, it was found that in the case of low-kV
CT scanning, the range of HNs was outside the
acceptable limits for potential dose errors.
(c)
Figure 3. Examples of inaccurate data transfer between the virtual References
simulator and the treatment planning system. (a) CT patient
1. Sherouse GW, Chaney EL. The portable virtual simulator.
orientation is reversed (a) head-first to feet-first, (b) supine to
Int J Radiation Oncol Biol Phys 1991; 21:475 481.
prone, and (c) all structure contours are drawn on the central
CT slice only. 2. McJury M, Dyker K, Nakielny R, Conway J,
Robinson MH. Optimizing localization accuracy in head
and neck, and brain radiotherapy. Br J Radiol 2006;
geometric coordinates. The CT scans were sent 79:672 680.
to the VS and contoured using the wire marker 3. McGee KP, Das IJ. Commissioning, acceptance testing,
pattern in the phantom, and a standard two- and quality assurance of a CT simulator. In: Coia LR,
Schultheiss TE, Hanks GE (eds). A Practical Guide to CT
field plan applied with known isocentre coordi- Simulation (pp. 5 23). Madison, Wisconsin: Advanced
nates, field setup shifts and DRRs. These struc- Medical Publishing, 1995.
tures and plans were then exported to the TPS 4. Mutic S, Palta JR, Butker EK, et al. Quality assurance for
and VARiS. The integrity of coordinates, struc- computed-tomography simulators and the computed-
tures and plan parameters were checked and tomography-simulation process: Report of the AAPM
found to be correct. Radiation Therapy Committee Task Group No. 66.
Med Phys 2003; 30 (10):2762 2792.
5. Aird E, Conway J. CT simulation for radiotherapy treat-
SUMMARY ment planning. Br J Radiol 2002; 75:1 13.
6. Conway J, Robinson MH. CT virtual simulation. Br J
We have presented a detailed report on the Radiol. 1997; 70:S106 S118.
commissioning tests performed on the mechan- 7. Craig T, Brochu D, Van Dyk J. A quality assurance
ical components of a new CT simulator (GE phantom for three-dimensional radiation treatment
161
Commissioning a new CT simulator I: CT simulator hardware
planning. Int J Radiation Oncol Biol Phys. 1999; 10. Kilby W, Sage J, Rabett V. Tolerance levels for quality
44:955 966. assurance of electron density values generated from CT
8. McGee KP, Das IJ, Sims C. Evaluation of digitally recon- in radiotherapy treatment planning. Phys Med Biol
structed radiographs (DRRs) used for clinical radiother- 2002; 47:1485 1492.
apy: A phantom study. Med Phys 1995; 22:1815 1827. 11. Knoos T, Nilsson M, Ahlgren L. A method for conversion
9. IPEM Report 91. Recommended Standards for the of Hounsfield number to electron density and prediction
Routine Performance Testing of Diagnostic X-ray Imaging of macroscopic pair production cross-sections. Rad Oncol
Systems. 2005. 1986; 5:337 345.
162
View publication stats
You might also like
- Hourglass Workout Program by Luisagiuliet 276% (21)Hourglass Workout Program by Luisagiuliet 251 pages
- Knee Ability Zero Now Complete As A Picture Book 4 PDF Free94% (68)Knee Ability Zero Now Complete As A Picture Book 4 PDF Free49 pages
- Read People Like A Book by Patrick King-Edited61% (70)Read People Like A Book by Patrick King-Edited12 pages
- Livingood, Blake - Livingood Daily Your 21-Day Guide To Experience Real Health77% (13)Livingood, Blake - Livingood Daily Your 21-Day Guide To Experience Real Health260 pages
- The 36 Questions That Lead To Love - The New York Times94% (34)The 36 Questions That Lead To Love - The New York Times3 pages
- The 36 Questions That Lead To Love - The New York Times95% (21)The 36 Questions That Lead To Love - The New York Times3 pages
- Jeffrey Epstein39s Little Black Book Unredacted PDF75% (12)Jeffrey Epstein39s Little Black Book Unredacted PDF95 pages
- 14 Easiest & Hardest Muscles To Build (Ranked With Solutions)100% (7)14 Easiest & Hardest Muscles To Build (Ranked With Solutions)27 pages
- The 4 Hour Workweek, Expanded and Updated by Timothy Ferriss - Excerpt23% (954)The 4 Hour Workweek, Expanded and Updated by Timothy Ferriss - Excerpt38 pages
- Quality Use of AI in Medical Imaging-What Do Radiologists Need To Know?No ratings yetQuality Use of AI in Medical Imaging-What Do Radiologists Need To Know?8 pages
- See, Think, and Act - Real-Time Adaptive Radiotherapy PDFNo ratings yetSee, Think, and Act - Real-Time Adaptive Radiotherapy PDF8 pages
- Design & Delivery of Automated Winston-Lutz Test For Isocentric &No ratings yetDesign & Delivery of Automated Winston-Lutz Test For Isocentric &66 pages
- Spesifikasi Teknis - ELEKTA MONACO Radiation Treatment Planning System (TPS)No ratings yetSpesifikasi Teknis - ELEKTA MONACO Radiation Treatment Planning System (TPS)1 page
- 312 Ncs Report 30 Qa of Brachytherapy With AfterloadersNo ratings yet312 Ncs Report 30 Qa of Brachytherapy With Afterloaders74 pages
- Comissioning and Verification of 10 MV Elekta Synergy Platform Linac Photon BeamNo ratings yetComissioning and Verification of 10 MV Elekta Synergy Platform Linac Photon Beam9 pages
- The Multileaf Collimator A Complete Guide James M. Galvin, DSC Thomas Jefferson University Hospital Jefferson Medical School Philadelphia, PaNo ratings yetThe Multileaf Collimator A Complete Guide James M. Galvin, DSC Thomas Jefferson University Hospital Jefferson Medical School Philadelphia, Pa17 pages
- Characteristics and Limitations of A Secondary Dose Check Software For VMAT Plan CalculationNo ratings yetCharacteristics and Limitations of A Secondary Dose Check Software For VMAT Plan Calculation8 pages
- Agility MLC Transmission Optimization in The MonacoNo ratings yetAgility MLC Transmission Optimization in The Monaco10 pages
- Dokumen - Tips Raphex 2001 Cloud Object Storage Store Retrieve Data s3 2012-04-30raphexNo ratings yetDokumen - Tips Raphex 2001 Cloud Object Storage Store Retrieve Data s3 2012-04-30raphex40 pages
- Get Clinical 3D Dosimetry in Modern Radiation Therapy 1st Edition Ben Mijnheer Free All Chapters100% (4)Get Clinical 3D Dosimetry in Modern Radiation Therapy 1st Edition Ben Mijnheer Free All Chapters62 pages
- 15° Wedge Transmission Factor CalculationNo ratings yet15° Wedge Transmission Factor Calculation10 pages
- Shielding Requirements in Helical Tomotherapy: Home Search Collections Journals About Contact Us My IopscienceNo ratings yetShielding Requirements in Helical Tomotherapy: Home Search Collections Journals About Contact Us My Iopscience12 pages
- Adaptive Radiotherapy For Bladder CancerNo ratings yetAdaptive Radiotherapy For Bladder Cancer12 pages
- Validation of A Virtual Source Model For Monte Carlo Dose Calculations of A FFF LinacNo ratings yetValidation of A Virtual Source Model For Monte Carlo Dose Calculations of A FFF Linac8 pages
- Dosimetric Effects of Multileaf Collimator Leaf Width On Intensity-ModulatedNo ratings yetDosimetric Effects of Multileaf Collimator Leaf Width On Intensity-Modulated11 pages
- Magnetic Resonance Only Workflow and Validation of Dose Calculations For Radiotherapy of Prostate CancerNo ratings yetMagnetic Resonance Only Workflow and Validation of Dose Calculations For Radiotherapy of Prostate Cancer6 pages
- Counting Statistics: Radiation Detect & Measure, Summer 2005 (RSM)No ratings yetCounting Statistics: Radiation Detect & Measure, Summer 2005 (RSM)15 pages
- History of Radiotherapy & Infrastructure in IndiaNo ratings yetHistory of Radiotherapy & Infrastructure in India106 pages
- Body MRI Artifacts in Clinical Practice: A Physicist's and Radiologist's PerspectiveNo ratings yetBody MRI Artifacts in Clinical Practice: A Physicist's and Radiologist's Perspective19 pages
- Summary From Tutorial SlicerRT and Dosimetry AnalysisNo ratings yetSummary From Tutorial SlicerRT and Dosimetry Analysis12 pages
- Download Complete Radiation Oncology A Question Based Review Borislav Hristov & Steven H Lin Md Phd & John P. Christodouleas Md Mph PDF for All Chapters100% (4)Download Complete Radiation Oncology A Question Based Review Borislav Hristov & Steven H Lin Md Phd & John P. Christodouleas Md Mph PDF for All Chapters24 pages
- Radiation Targets 1: DNA, Chromosome and Chromatid Damage and RepairNo ratings yetRadiation Targets 1: DNA, Chromosome and Chromatid Damage and Repair71 pages
- Image Registration, Deformation, and Enhanced Contouring For Radiotherapy With MIM MaestroNo ratings yetImage Registration, Deformation, and Enhanced Contouring For Radiotherapy With MIM Maestro16 pages
- Use of Image Registration and Fusion Algorithms and Techniques in Radiotherapy - Report of The AAPM Radiation Therapy Committee Task Group No. 132No ratings yetUse of Image Registration and Fusion Algorithms and Techniques in Radiotherapy - Report of The AAPM Radiation Therapy Committee Task Group No. 13235 pages
- Calibration of Dosimeters Used in Radiation Therapy100% (2)Calibration of Dosimeters Used in Radiation Therapy122 pages
- Comparison of Different Number of Beams in Intensity Modulated Radiotherapy in Head and Neck CancerNo ratings yetComparison of Different Number of Beams in Intensity Modulated Radiotherapy in Head and Neck Cancer11 pages
- Independent Dose Calculations Concepts and ModelsNo ratings yetIndependent Dose Calculations Concepts and Models104 pages
- Brachytherapy Systems, Remote AfterloadingNo ratings yetBrachytherapy Systems, Remote Afterloading24 pages
- Comprehensive Audits of Radiotherapy Practices: A Tool for Quality ImprovementFrom EverandComprehensive Audits of Radiotherapy Practices: A Tool for Quality ImprovementNo ratings yet
- Radiotherapy in Clinical Practice, second edition: A Pocket GuideFrom EverandRadiotherapy in Clinical Practice, second edition: A Pocket GuideNo ratings yet
- Understanding the challenges of delivering radiotherapy in low- andNo ratings yetUnderstanding the challenges of delivering radiotherapy in low- and8 pages
- Victims in The Dark Shadows A Model of Toxic Leadership. JournalNo ratings yetVictims in The Dark Shadows A Model of Toxic Leadership. Journal13 pages
- A Study of Base Isolation System at Cyclotron BuilNo ratings yetA Study of Base Isolation System at Cyclotron Buil9 pages
- Radiation Exposure and Image Quality in X-Ray Diagnostic Radiology Physical Principles and Clinical Applications (PDFDrive)No ratings yetRadiation Exposure and Image Quality in X-Ray Diagnostic Radiology Physical Principles and Clinical Applications (PDFDrive)208 pages
- Beam Modification Devices in Radiotherapy 3No ratings yetBeam Modification Devices in Radiotherapy 345 pages
- Example On Infection Control - Failure Modes and Effects Analysis Tool Process Data ReportNo ratings yetExample On Infection Control - Failure Modes and Effects Analysis Tool Process Data Report2 pages
- 16-C110518B-Svb Eqx 2058 Addis Ababa University, EthiopiaNo ratings yet16-C110518B-Svb Eqx 2058 Addis Ababa University, Ethiopia1 page
- Radiotherapy Scheduling: Abstract. This Chapter Concerns Radiotherapy Scheduling Problems Identified atNo ratings yetRadiotherapy Scheduling: Abstract. This Chapter Concerns Radiotherapy Scheduling Problems Identified at35 pages
- Petroltecnica Environmental Services Pre Qualification DocumentsNo ratings yetPetroltecnica Environmental Services Pre Qualification Documents55 pages
- Chi2 Feature Selection and Discretization of Numeric AttributesNo ratings yetChi2 Feature Selection and Discretization of Numeric Attributes4 pages
- Oil Spill Response Field Manual - 2014 - E PDF100% (1)Oil Spill Response Field Manual - 2014 - E PDF368 pages
- ME3112 8 Planar Mechanisms - Solved Examples - 16102014133235158No ratings yetME3112 8 Planar Mechanisms - Solved Examples - 1610201413323515817 pages





















































































































- Knee Ability Zero Now Complete As A Picture Book 4 PDF FreeKnee Ability Zero Now Complete As A Picture Book 4 PDF Free
- Livingood, Blake - Livingood Daily Your 21-Day Guide To Experience Real HealthLivingood, Blake - Livingood Daily Your 21-Day Guide To Experience Real Health
- The 36 Questions That Lead To Love - The New York TimesThe 36 Questions That Lead To Love - The New York Times
- The 36 Questions That Lead To Love - The New York TimesThe 36 Questions That Lead To Love - The New York Times
- Jeffrey Epstein39s Little Black Book Unredacted PDFJeffrey Epstein39s Little Black Book Unredacted PDF
- 14 Easiest & Hardest Muscles To Build (Ranked With Solutions)14 Easiest & Hardest Muscles To Build (Ranked With Solutions)
- The 4 Hour Workweek, Expanded and Updated by Timothy Ferriss - ExcerptThe 4 Hour Workweek, Expanded and Updated by Timothy Ferriss - Excerpt
- Quality Use of AI in Medical Imaging-What Do Radiologists Need To Know?Quality Use of AI in Medical Imaging-What Do Radiologists Need To Know?
- See, Think, and Act - Real-Time Adaptive Radiotherapy PDFSee, Think, and Act - Real-Time Adaptive Radiotherapy PDF
- Design & Delivery of Automated Winston-Lutz Test For Isocentric &Design & Delivery of Automated Winston-Lutz Test For Isocentric &
- Spesifikasi Teknis - ELEKTA MONACO Radiation Treatment Planning System (TPS)Spesifikasi Teknis - ELEKTA MONACO Radiation Treatment Planning System (TPS)
- 312 Ncs Report 30 Qa of Brachytherapy With Afterloaders312 Ncs Report 30 Qa of Brachytherapy With Afterloaders
- Comissioning and Verification of 10 MV Elekta Synergy Platform Linac Photon BeamComissioning and Verification of 10 MV Elekta Synergy Platform Linac Photon Beam
- The Multileaf Collimator A Complete Guide James M. Galvin, DSC Thomas Jefferson University Hospital Jefferson Medical School Philadelphia, PaThe Multileaf Collimator A Complete Guide James M. Galvin, DSC Thomas Jefferson University Hospital Jefferson Medical School Philadelphia, Pa
- Characteristics and Limitations of A Secondary Dose Check Software For VMAT Plan CalculationCharacteristics and Limitations of A Secondary Dose Check Software For VMAT Plan Calculation
- Agility MLC Transmission Optimization in The MonacoAgility MLC Transmission Optimization in The Monaco
- Dokumen - Tips Raphex 2001 Cloud Object Storage Store Retrieve Data s3 2012-04-30raphexDokumen - Tips Raphex 2001 Cloud Object Storage Store Retrieve Data s3 2012-04-30raphex
- Get Clinical 3D Dosimetry in Modern Radiation Therapy 1st Edition Ben Mijnheer Free All ChaptersGet Clinical 3D Dosimetry in Modern Radiation Therapy 1st Edition Ben Mijnheer Free All Chapters
- Shielding Requirements in Helical Tomotherapy: Home Search Collections Journals About Contact Us My IopscienceShielding Requirements in Helical Tomotherapy: Home Search Collections Journals About Contact Us My Iopscience
- Validation of A Virtual Source Model For Monte Carlo Dose Calculations of A FFF LinacValidation of A Virtual Source Model For Monte Carlo Dose Calculations of A FFF Linac
- Dosimetric Effects of Multileaf Collimator Leaf Width On Intensity-ModulatedDosimetric Effects of Multileaf Collimator Leaf Width On Intensity-Modulated
- Magnetic Resonance Only Workflow and Validation of Dose Calculations For Radiotherapy of Prostate CancerMagnetic Resonance Only Workflow and Validation of Dose Calculations For Radiotherapy of Prostate Cancer
- Counting Statistics: Radiation Detect & Measure, Summer 2005 (RSM)Counting Statistics: Radiation Detect & Measure, Summer 2005 (RSM)
- Body MRI Artifacts in Clinical Practice: A Physicist's and Radiologist's PerspectiveBody MRI Artifacts in Clinical Practice: A Physicist's and Radiologist's Perspective
- Summary From Tutorial SlicerRT and Dosimetry AnalysisSummary From Tutorial SlicerRT and Dosimetry Analysis
- Download Complete Radiation Oncology A Question Based Review Borislav Hristov & Steven H Lin Md Phd & John P. Christodouleas Md Mph PDF for All ChaptersDownload Complete Radiation Oncology A Question Based Review Borislav Hristov & Steven H Lin Md Phd & John P. Christodouleas Md Mph PDF for All Chapters
- Radiation Targets 1: DNA, Chromosome and Chromatid Damage and RepairRadiation Targets 1: DNA, Chromosome and Chromatid Damage and Repair
- Image Registration, Deformation, and Enhanced Contouring For Radiotherapy With MIM MaestroImage Registration, Deformation, and Enhanced Contouring For Radiotherapy With MIM Maestro
- Use of Image Registration and Fusion Algorithms and Techniques in Radiotherapy - Report of The AAPM Radiation Therapy Committee Task Group No. 132Use of Image Registration and Fusion Algorithms and Techniques in Radiotherapy - Report of The AAPM Radiation Therapy Committee Task Group No. 132
- Calibration of Dosimeters Used in Radiation TherapyCalibration of Dosimeters Used in Radiation Therapy
- Comparison of Different Number of Beams in Intensity Modulated Radiotherapy in Head and Neck CancerComparison of Different Number of Beams in Intensity Modulated Radiotherapy in Head and Neck Cancer
- Innovative Radiotherapy Techniques for Prostate CancerFrom EverandInnovative Radiotherapy Techniques for Prostate Cancer
- Comprehensive Audits of Radiotherapy Practices: A Tool for Quality ImprovementFrom EverandComprehensive Audits of Radiotherapy Practices: A Tool for Quality Improvement
- Radiotherapy in Clinical Practice, second edition: A Pocket GuideFrom EverandRadiotherapy in Clinical Practice, second edition: A Pocket Guide
- Understanding the challenges of delivering radiotherapy in low- andUnderstanding the challenges of delivering radiotherapy in low- and
- Victims in The Dark Shadows A Model of Toxic Leadership. JournalVictims in The Dark Shadows A Model of Toxic Leadership. Journal
- A Study of Base Isolation System at Cyclotron BuilA Study of Base Isolation System at Cyclotron Buil
- Radiation Exposure and Image Quality in X-Ray Diagnostic Radiology Physical Principles and Clinical Applications (PDFDrive)Radiation Exposure and Image Quality in X-Ray Diagnostic Radiology Physical Principles and Clinical Applications (PDFDrive)
- Example On Infection Control - Failure Modes and Effects Analysis Tool Process Data ReportExample On Infection Control - Failure Modes and Effects Analysis Tool Process Data Report
- 16-C110518B-Svb Eqx 2058 Addis Ababa University, Ethiopia16-C110518B-Svb Eqx 2058 Addis Ababa University, Ethiopia
- Radiotherapy Scheduling: Abstract. This Chapter Concerns Radiotherapy Scheduling Problems Identified atRadiotherapy Scheduling: Abstract. This Chapter Concerns Radiotherapy Scheduling Problems Identified at
- Petroltecnica Environmental Services Pre Qualification DocumentsPetroltecnica Environmental Services Pre Qualification Documents
- Chi2 Feature Selection and Discretization of Numeric AttributesChi2 Feature Selection and Discretization of Numeric Attributes
- ME3112 8 Planar Mechanisms - Solved Examples - 16102014133235158ME3112 8 Planar Mechanisms - Solved Examples - 16102014133235158