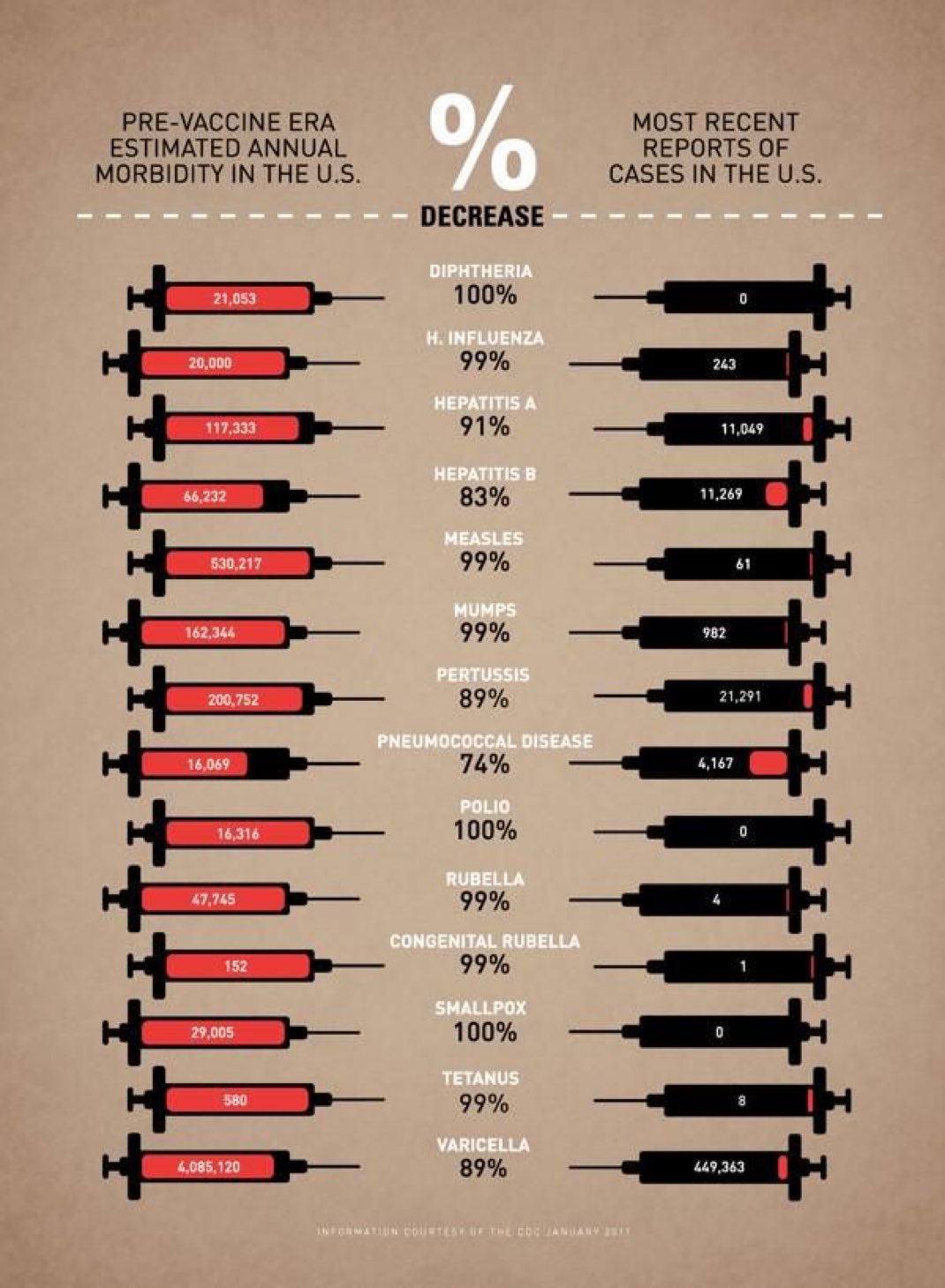
History tells us vaccines are wonderful things. Vaccines cut horrible, disifiguring, crippling and fatal diseases, and extended the life span of entire populations across the entire world.
World Malaria Report 2020 carries bad news. Despite remarkable progress against malaria, despite being on the verge of beating the disease and eradicating it from the planet, governments stopped supporting anti-malaria work.
Malaria is poised to come roaring back to kill millions.
COVID-19 complicates fighting malaria. But the real enemy of the fight against malaria is apathy, neglect and ignorance.
Cover of World Malaria Report 2020, WHO’s annual accounting of the fight to eradicate malaria.
WHO calls for reinvigorated action to fight malaria
Global malaria gains threatened by access gaps, COVID-19 and funding shortfalls
30 November 2020
News release
Reading time: 6 min(1645 words)
The World Health Organization (WHO) is calling on countries and global health partners to step up the fight against malaria, a preventable and treatable disease that continues to claim hundreds of thousands of lives each year. A better targeting of interventions, new tools and increased funding are needed to change the global trajectory of the disease and reach internationally-agreed targets.
According to WHO‘s latest World malaria report, progress against malaria continues to plateau, particularly in high burden countries in Africa. Gaps in access to life-saving tools are undermining global efforts to curb the disease, and the COVID-19 pandemic is expected to set back the fight even further.
“It is time for leaders across Africa – and the world – to rise once again to the challenge of malaria, just as they did when they laid the foundation for the progress made since the beginning of this century,” said WHO Director-General Dr Tedros Adhanom Ghebreyesus. “Through joint action, and a commitment to leaving no one behind, we can achieve our shared vision of a world free of malaria.”
In 2000, African leaders signed the landmark Abuja Declaration pledging to reduce malaria deaths on the continent by 50% over a 10-year period. Robust political commitment, together with innovations in new tools and a steep increase in funding, catalyzed an unprecedented period of success in global malaria control. According to the report, 1.5 billion malaria cases and 7.6 million deaths have been averted since 2000.
A plateau in progress
In 2019, the global tally of malaria cases was 229 million, an annual estimate that has remained virtually unchanged over the last 4 years. The disease claimed some 409 000 lives in 2019 compared to 411 000 in 2018.
As in past years, the African Region shouldered more than 90% of the overall disease burden. Since 2000, the region has reduced its malaria death toll by 44%, from an estimated 680 000 to 384 000 annually. However, progress has slowed in recent years, particularly in countries with a high burden of the disease.
A funding shortfall at both the international and domestic levels poses a significant threat to future gains. In 2019, total funding reached US $3 billion against a global target of $5.6 billion. Funding shortages have led to critical gaps in access to proven malaria control tools.
COVID-19 an added challenge
In 2020, COVID-19 emerged as an additional challenge to the provision of essential health services worldwide. According to the report, most malaria prevention campaigns were able to move forward this year without major delays. Ensuring access to malaria prevention – such as insecticide-treated nets and preventive medicines for children – has supported the COVID-19 response strategy by reducing the number of malaria infections and, in turn, easing the strain on health systems. WHO worked swiftly to provide countries with guidance to adapt their responses and ensure the safe delivery of malaria services during the pandemic.
However, WHO is concerned that even moderate disruptions in access to treatment could lead to a considerable loss of life. The report finds, for example, that a 10% disruption in access to effective antimalarial treatment in sub-Saharan Africa could lead to 19 000 additional deaths. Disruptions of 25% and 50% in the region could result in an additional 46 000 and 100 000 deaths, respectively.
“While Africa has shown the world what can be achieved if we stand together to end malaria as a public health threat, progress has stalled,” said Dr Matshidiso Moeti, WHO Regional Director for Africa. “COVID-19 threatens to further derail our efforts to overcome malaria, particularly treating people with the disease. Despite the devastating impact COVID-19 has had on African economies, international partners and countries need to do more to ensure that the resources are there to expand malaria programmes which are making such a difference in people’s lives.”
WHO response
A key strategy to reignite progress is the “High burden to high impact” (HBHI) response, catalyzed in 2018 by WHO and the RBM Partnership to End Malaria. The response is led by 11 countries – including 10 in sub-Saharan Africa – that account for approximately 70% of the world’s malaria burden.
Over the last 2 years, HBHI countries have been moving away from a “one-size-fits all” approach to malaria control – opting, instead, for tailored responses based on local data and intelligence. A recent analysis from Nigeria, for example, found that through an optimized mix of interventions, the country could avert tens of millions of additional cases and thousands of additional deaths by the year 2023, compared to a business-as-usual approach.
While it is too early to measure the impact of the HBHI approach, the report finds that deaths in the 11 countries were reduced from 263 000 to 226 000 between 2018 and 2019. India continued to make impressive gains, with reductions in cases and deaths of 18% and 20%, respectively, over the last 2 years. There was, however, a slight increase in the total number of cases among HBHI countries, from an estimated 155 million in 2018 to 156 million in 2019.
Meeting global malaria targets
This year’s report highlights key milestones and events that helped shape the global response to the disease in recent decades. Beginning in the 1990s, leaders of malaria-affected countries, scientists and other partners laid the groundwork for a renewed malaria response that contributed to one of the biggest returns on investment in global health.
According to the report, 21 countries eliminated malaria over the last 2 decades; of these, 10 countries were officially certified as malaria-free by WHO. In the face of the ongoing threat of antimalarial drug resistance, the 6 countries of the Greater Mekong subregion continue to make major gains towards their goal of malaria elimination by 2030.
But many countries with a high burden of malaria have been losing ground. According to WHO global projections, the 2020 target for reductions in malaria case incidence will be missed by 37% and the mortality reduction target will be missed by 22%.
Note to editors
WHO’s work on malaria is guided by the Global technical strategy for malaria 2016-2030 (GTS), approved by the World Health Assembly in May 2015. The strategy includes four global targets for 2030, with milestones along the way to track progress. The 2030 targets are: 1) reducing malaria case incidence by at least 90%; 2) reducing malaria mortality rates by at least 90%; 3) eliminating malaria in at least 35 countries; and
4) preventing a resurgence of malaria in all countries that are malaria-free.
Near-term GTS milestones for 2020 include global reductions in malaria case incidence and death rates of at least 40% and the elimination of malaria in at least 10 countries. According to the report, the 2020 milestones for malaria case incidence and mortality rates will be missed:
– Case incidence: WHO projects that, in 2020, there were an estimated 56 malaria cases for every 1000 people at risk of the disease against a GTS target of 35 cases. The GTS milestone will be missed by an estimated 37%.
– Mortality rate: The estimate for globally projected malaria deaths per 100 000 population at risk was 9.8 in 2020 against a GTS target of 7.2 deaths. The milestone will be missed by an estimated 22%.
WHO African Region – Since 2014, the rate of progress in both cases and deaths in the region has slowed, attributed mainly to the stalling of progress in several countries with moderate or high transmission. In 2019, six African countries accounted for 50% of all malaria cases globally: Nigeria (23%), the Democratic Republic of the Congo (11%), United Republic of Tanzania (5%), Niger (4%), Mozambique (4%) and Burkina Faso (4%). In view of recent trends, the African Region will miss the GTS 2020 milestones for case incidence and mortality by 37% and 25%, respectively.
“High burden to high impact” (HBHI) – Launched in November 2018, HBHI builds on the principle that no one should die from a disease that is preventable and treatable. It is led by 11 countries that, together, accounted for approximately 70% of the world’s malaria burden in 2017: Burkina Faso, Cameroon, Democratic Republic of the Congo, Ghana, India, Mali, Mozambique, Niger, Nigeria, Uganda and United Republic of Tanzania. Over the last two years, all 11 HBHI countries have implemented activities across four response elements: 1) political will to reduce the toll of malaria; 2) strategic information to drive impact; 3) better guidance, policies and strategies; and 4) a coordinated national malaria response
Malaria elimination – Between 2000 and 2019, 10 countries received the official WHO certification of malaria elimination: United Arab Emirates (2007), Morocco (2010), Turkmenistan (2010), Armenia (2011), Kyrgyzstan (2016), Sri Lanka (2016), Uzbekistan (2018), Paraguay (2018), Argentina (2019) and Algeria (2019). In 2019, China reported zero indigenous cases of malaria for the third consecutive year; the country recently applied for the official WHO certification of malaria elimination. In 2020, El Salvador became the first country in Central America to apply for the WHO malaria-free certification
In the six countries of the Greater Mekong subregion – Cambodia, China (Yunnan Province), Lao People’s Democratic Republic, Myanmar, Thailand and Viet Nam – the reported number of malaria cases fell by 90% from 2000 to 2019, while P. falciparum (Pf) cases fell by 97% in the same time period. This accelerated decrease in Pf malaria is notable in view of the threat posed by antimalarial drug resistance in the subregion.
A call for innovation – Eliminating malaria in all countries, especially those with a high disease burden, will likely require tools that are not available today. In September 2019, the WHO Director-General issued a “malaria challenge,” calling on the global health community to ramp up investment in the research and development of new malaria-fighting tools and approaches. This message was further reinforced in the April 2020 report of the WHO Strategic advisory group on malaria eradication.
Spread the word; friends don't allow friends to repeat history.
Covers of the last four World Malaria Reports. World Health Organization (WHO)
It’s a common tale but true: In any period when nations collaborate to defeat or eradicate malaria, funders of the programs get board and cut funding.
Malaria roars back.
This cycle has nothing to do with pesticides or medicines, mostly. Especially it’s not a problem that can be fixed with more DDT.
When a nation focuses on beating malaria, progress occurs. When nations lose their focus, malaria strikes back.
After great progress reducing malaria infections and malaria deaths between 1999 and 2017, nations including the U.S. lost focus. International donors failed to contribute enough money to keep the fight going.
World Malaria Report 2018 notes the striking back by malaria.
One other thing we can be quite sure of: Almost all mass media will ignore this report.
What will you do to change things?
You can help by donating $10 to a charity that delivers bednets to people who need them in Asia and Africa. You can help by writing letters to your local newspapers, to your Congressional representatives, and to the President. Every little bit helps.
Here’s the press release on World Malaria Report 2018, which was released by the World Health Organization (WHO) on November 19, 2018.
WHO and partners launch new country-led response to put stalled malaria control efforts back on track
19 November 2018
News Release
Maputo/Geneva
Reductions in malaria cases have stalled after several years of decline globally, according to the new World malaria report 2018. To get the reduction in malaria deaths and disease back on track, WHO and partners are joining a new country-led response, launched today, to scale up prevention and treatment, and increased investment, to protect vulnerable people from the deadly disease.
For the second consecutive year, the annual report produced by WHO reveals a plateauing in numbers of people affected by malaria: in 2017, there were an estimated 219 million cases of malaria, compared to 217 million the year before. But in the years prior, the number of people contracting malaria globally had been steadily falling, from 239 million in 2010 to 214 million in 2015.
“Nobody should die from malaria. But the world faces a new reality: as progress stagnates, we are at risk of squandering years of toil, investment and success in reducing the number of people suffering from the disease,” says Dr Tedros Adhanom Ghebreyesus, WHO Director-General. “We recognise we have to do something different – now. So today we are launching a country-focused and -led plan to take comprehensive action against malaria by making our work more effective where it counts most – at local level.”
Where malaria is hitting hardest
In 2017, approximately 70% of all malaria cases (151 million) and deaths (274 000) were concentrated in 11 countries: 10 in Africa (Burkina Faso, Cameroon, Democratic Republic of the Congo, Ghana, Mali, Mozambique, Niger, Nigeria, Uganda and United Republic of Tanzania) and India. There were 3.5 million more malaria cases reported in these 10 African countries in 2017 compared to the previous year, while India, however, showed progress in reducing its disease burden.
Despite marginal increases in recent years in the distribution and use of insecticide-treated bed nets in sub-Saharan Africa – the primary tool for preventing malaria – the report highlights major coverage gaps. In 2017, an estimated half of at-risk people in Africa did not sleep under a treated net. Also, fewer homes are being protected by indoor residual spraying than before, and access to preventive therapies that protect pregnant women and children from malaria remains too low.
High impact response needed
In line with WHO’s strategic vision to scale up activities to protect people’s health, the new country-driven “High burden to high impact” response plan has been launched to support nations with most malaria cases and deaths. The response follows a call made by Dr Tedros at the World Health Assembly in May 2018 for an aggressive new approach to jump-start progress against malaria. It is based on four pillars:
Galvanizing national and global political attention to reduce malaria deaths;
Driving impact through the strategic use of information;
Establishing best global guidance, policies and strategies suitable for all malaria endemic countries; and
Implementing a coordinated country response.
Catalyzed by WHO and the RBM Partnership to End Malaria, “High burden to high impact” builds on the principle that no one should die from a disease that can be easily prevented and diagnosed, and that is entirely curable with available treatments.
“There is no standing still with malaria. The latest World malaria report shows that further progress is not inevitable and that business as usual is no longer an option,” said Dr Kesete Admasu, CEO of the RBM Partnership. “The new country-led response will jumpstart aggressive new malaria control efforts in the highest burden countries and will be crucial to get back on track with fighting one of the most pressing health challenges we face.”
Targets set by the WHO Global technical strategy for malaria 2016–2030 to reduce malaria case incidence and death rates by at least 40% by 2020 are not on track to being met.
Pockets of progress
The report highlights some positive progress. The number of countries nearing elimination continues to grow (46 in 2017 compared to 37 in 2010). Meanwhile in China and El Salvador, where malaria had long been endemic, no local transmission of malaria was reported in 2017, proof that intensive, country-led control efforts can succeed in reducing the risk people face from the disease.
In 2018, WHO certified Paraguay as malaria free, the first country in the Americas to receive this status in 45 years. Three other countries – Algeria, Argentina and Uzbekistan – have requested official malaria-free certification from WHO.
India – a country that represents 4% of the global malaria burden – recorded a 24% reduction in cases in 2017 compared to 2016. Also in Rwanda, 436 000 fewer cases were recorded in 2017 compared to 2016. Ethiopia and Pakistan both had estimated decreases of more than 240 000 in the same period.
“When countries prioritize action on malaria, we see the results in lives saved and cases reduced,” says Dr Matshidiso Moeti, WHO Regional Director for Africa. “WHO and global malaria control partners will continue striving to help governments, especially those with the highest burden, scale up the response to malaria.”
Domestic financing is key
As reductions in malaria cases and deaths slow, funding for the global response has also shown a levelling off, with US$ 3.1 billion made available for control and elimination programmes in 2017 including US$ 900 million (28%) from governments of malaria endemic countries. The United States of America remains the largest single international donor, contributing US$ 1.2 billion (39%) in 2017.
To meet the 2030 targets of the global malaria strategy, malaria investments should reach at least US$6.6 billion annually by 2020 – more than double the amount available today.
29 November 2017 | Geneva – After unprecedented global success in malaria control, progress has stalled, according to the World malaria report 2017. There were an estimated 5 million more malaria cases in 2016 than in 2015. Malaria deaths stood at around 445 000, a similar number to the previous year.
“In recent years, we have made major gains in the fight against malaria,” said Dr Tedros Adhanom Ghebreyesus, Director-General of WHO. “We are now at a turning point. Without urgent action, we risk going backwards, and missing the global malaria targets for 2020 and beyond.”
The WHO Global Technical Strategy for Malaria calls for reductions of at least 40% in malaria case incidence and mortality rates by the year 2020. According to WHO’s latest malaria report, the world is not on track to reach these critical milestones.
A major problem is insufficient funding at both domestic and international levels, resulting in major gaps in coverage of insecticide-treated nets, medicines, and other life-saving tools.
Funding shortage
An estimated US$ 2.7 billion was invested in malaria control and elimination efforts globally in 2016. That is well below the US $6.5 billion annual investment required by 2020 to meet the 2030 targets of the WHO global malaria strategy.
In 2016, governments of endemic countries provided US$ 800 million, representing 31% of total funding. The United States of America was the largest international funder of malaria control programmes in 2016, providing US$1 billion (38% of all malaria funding), followed by other major donors, including the United Kingdom of Great Britain and Northern Ireland, France, Germany and Japan.
The global figures
The report shows that, in 2016, there were an estimated 216 million cases of malaria in 91 countries, up from 211 million cases in 2015. The estimated global tally of malaria deaths reached 445 000 in 2016 compared to 446 000 the previous year.
While the rate of new cases of malaria had fallen overall, since 2014 the trend has levelled off and even reversed in some regions. Malaria mortality rates followed a similar pattern.
The African Region continues to bear an estimated 90% of all malaria cases and deaths worldwide. Fifteen countries – all but one in sub-Saharan Africa – carry 80% of the global malaria burden.
“Clearly, if we are to get the global malaria response back on track, supporting the most heavily affected countries in the African Region must be the primary focus,” said Dr Tedros.
Controlling malaria
In most malaria-affected countries, sleeping under an insecticide-treated bednet (ITN) is the most common and most effective way to prevent infection. In 2016, an estimated 54% of people at risk of malaria in sub-Saharan Africa slept under an ITN compared to 30% in 2010. However, the rate of increase in ITN coverage has slowed since 2014, the report finds.
Spraying the inside walls of homes with insecticides is another effective way to prevent malaria. The report reveals a steep drop in the number of people protected from malaria by this method – from an estimated 180 million in 2010 to 100 million in 2016 – with the largest reductions seen in the African Region.
The African Region has seen a major increase in diagnostic testing in the public health sector: from 36% of suspected cases in 2010 to 87% in 2016. A majority of patients (70%) who sought treatment for malaria in the public health sector received artemisinin-based combination therapies (ACTs) – the most effective antimalarial medicines.
However, in many areas, access to the public health system remains low. National-level surveys in the African Region show that only about one third (34%) of children with a fever are taken to a medical provider in the public health sector.
Tackling malaria in complex settings
The report also outlines additional challenges in the global malaria response, including the risks posed by conflict and crises in malaria endemic zones. WHO is currently supporting malaria responses in Nigeria, South Sudan, Venezuela (Bolivarian Republic of) and Yemen, where ongoing humanitarian crises pose serious health risks. In Nigeria’s Borno State, for example, WHO supported the launch of a mass antimalarial drug administration campaign this year that reached an estimated 1.2 million children aged under 5 years in targeted areas. Early results point to a reduction in malaria cases and deaths in this state.
A wake-up call
“We are at a crossroads in the response to malaria,” said Dr Pedro Alonso, Director of the Global Malaria Programme, commenting on the findings of this year’s report. “We hope this report serves as a wake-up call for the global health community. Meeting the global malaria targets will only be possible through greater investment and expanded coverage of core tools that prevent, diagnose and treat malaria. Robust financing for the research and development of new tools is equally critical.”
Details of DDT use in the past year usually show up in the bowels of the report.
Spread the word; friends don't allow friends to repeat history.
Mozambique’s National Malaria Control Programme distributed 4 million LLIN, insecticide-impregnated nets, to protect children and others from malaria as they sleep, the time most malaria-infecting mosquito bites occur. Malaria Consortium photo
But DDT’s effectiveness diminishes rapidly, as does the effectiveness of the other eleven insecticides generally used for IRS against malaria or other vector-borne diseases. Insecticides are sprayed indoors, and not outdoors, to provide protection where humans are most often bitten, and to prevent non-target mosquitoes and other creatures from being exposed to the insecticides. This prevents harmful pests from developing resistance to the insecticides, and diminishes damage to beneficial species, like food fish.
Instead of spraying, malaria fighters turn increasingly to bednets impregnated with insecticide, known as Long-Lasting Insecticide-impregnated Nets (LLIN). A net provides closer to 100% protection from bites than IRS. A net immediately protects anyone sleeping under it, while IRS must treat at least 80% of nearby homes to achieve more than 50 percent prevention.
While still using IRS, Mozambique stakes its future malaria fighting on nets.
Malaria Consortium has successfully completed a mass distribution campaign of over four million long-lasting insecticidal nets (LLINs) across Nampula and Niassa provinces in Mozambique. The nets were distributed almost simultaneously across all districts of each province – 23 districts in Nampula in November 2016, and 16 districts in Niassa in May 2017 – using a new operational model aimed at optimising resources.
Throughout the campaigns, Mozambique’s National Malaria Control Programme was responsible for the LLIN acquisition and led overall planning and implementation through the decentralised structures of the health system. Malaria Consortium’s role consisted of operational support, which included financial management, transport, procurement, logistics, training, management of service providers, efficient use of resources and effective coordination at provincial, district and field levels.
Sonia Gwesela, Malaria Consortium Mozambique Country Director said, “In Nampula Province, a major achievement was that 99 percent of households collected their nets. We successfully delivered 98 percent of the nets in both provinces, coming well above the 90 percent target set by the National Malaria Control Programme.
“With the successful completion of the distribution, we can now focus on a post-distribution communications campaign about the correct use of LLINs,” she concluded.
Bednets can be twice as effective as IRS in preventing the spread of malaria. Beating malaria also requires upgrading health care for quick diagnoses and quick, complete treatment of malaria in humans, and prevention projects to drain mosquito-breeding places within 50 yards of homes; more prevention of bites means less medical treatment is required.
WHO estimated 5 million people died of malaria in the 1950s into the 1960s. WHO’s Malaria Report 2016 reported malaria deaths fell to less than 430,000 world wide, a more than 90 percent reduction since 1963, mostly accomplished without DDT.
Cullen Crawford posted this on Twitter: “We dip our toes into depressing images on this site but nothing no approaches these torn up lotto ticket on floor of emergency room triage.”
If America is a just and true nation, the Affordable Care Act will be strengthened, not repealed to redistribute wealth to rich guys.
A woman shows the mosquito net that protects her and her family from malaria transmission, in India. India remains the world’s top DDT user, but is switching to nets in an effort to bring malaria rates down and set up malaria eradication before the end of DDT in 2020. WHO image.
World Health Organization publishes an annual World Malaria Report, with the year appended to the title. It summarizes the state of the fight against malaria worldwide, recording progress and setbacks.
In the tally of progress we get a clear indication of what is needed to continue or increase that progress, with the ultimate goal of controlling malaria to the point it poses no great economic risk, or health risk, to any nation, or better that human malaria is eradicated.
World Malaria Report 2016 is 184 pages, shorter than some previous reports but packed with figures and history, some of which requires greater background to understand completely.
For example, the 2016 publication notes that about 412,000 people died from malaria in 2016. This is a shocking figure. Most of the news coverage of the report mentions this death toll in the first paragraph.
It’s too many deaths. But it’s a more than 50% reduction in deaths from 1990s rates, and it’s a more than 90% reduction from the annual death tolls that shocked the world to concerted action after World War II. Most estimates are that about 5 million people a year died from malaria through the 1950s, and into the 1960s.
WHO concentrates on the malaria fight, and plays down the political aspects to encourage international cooperation to help fight the disease. But there are political statements made, if one has the background to understand them. There remains controversy over the use of DDT, with many people yelling far and wide that if ‘bans on DDT were removed’ then malaria would quickly become an eradicated disease. This position ignores the facts, that there were still 5 million people dying each year during peak DDT use; that death tolls plunged after the U.S. banned DDT use on crops; that the U.S. ban covered only crop use, and that DDT use against disease has never been banned anywhere in the world; and that DDT use continued long after the U.S. banned DDT, around the world. DDT use never stopped.
Taken together, we would understand that the 90% reduction in malaria deaths from peak DDT use years, was accomplished mostly without DDT, and that therefore DDT is not a panacea.
World Malaria Report 2016 also tallies the slow demise of DDT. Mosquito resistance to pesticides, especially DDT, is a major problem in the fight against the disease. But more DDT can’t fix that problem now that every mosquito on Earth carries alleles that make them resistant and wholly immune to the stuff. DDT will probably never be a panacea, even were its manufacture not scheduled to stop very soon.
History, and a complete assessment of the science and current conditions in the frontlines of the malaria fight, can help us put these things in perspective.
So far, only the Los Angeles Times in the U.S. provided any in-depth reporting on World Malaria Report 2016. We hope other media will take up the challenge to inform. They will find WHO’s Fact Sheet useful.
With that warning in mind, it’s good to look at the broad outlines of the report, which WHO has packaged into a fact sheet for our convenience.
Fact Sheet: World Malaria Report 2016
13 December 2016
The World Malaria Report, published annually by WHO, tracks progress and trends in malaria control and elimination across the globe. It is developed by WHO in collaboration with ministries of health and a broad range of partners. The 2016 report draws on data from 91 countries and areas with ongoing malaria transmission.
According to the report, there were 212 million new cases of malaria worldwide in 2015 (range 148–304 million). The WHO African Region accounted for most global cases of malaria (90%), followed by the South-East Asia Region (7%) and the Eastern Mediterranean Region (2%).
In 2015, there were an estimated 429 000 malaria deaths (range 235 000–639 000) worldwide. Most of these deaths occurred in the African Region (92%), followed by the South-East Asia Region (6%) and the Eastern Mediterranean Region (2%).
Between 2010 and 2015, malaria incidence rates (new malaria cases) fell by 21% globally and in the African Region. During this same period, malaria mortality rates fell by an estimated 29% globally and by 31% in the African Region.
Between 2010 and 2015, malaria incidence rates (new malaria cases) fell by 21% globally and in the African Region. During this same period, malaria mortality rates fell by an estimated 29% globally and by 31% in the African Region.
Other regions have achieved impressive reductions in their malaria burden. Since 2010, the malaria mortality rate declined by 58% in the Western Pacific Region, by 46% in the South-East Asia Region, by 37% in the Region of the Americas and by 6% in the Eastern Mediterranean Region. In 2015, the European Region was malaria-free: all 53 countries in the region reported at least 1 year of zero locally-acquired cases of malaria.
Children under 5 are particularly susceptible to malaria illness, infection and death. In 2015, malaria killed an estimated 303 000 under-fives globally, including 292 000 in the African Region. Between 2010 and 2015, the malaria mortality rate among children under 5 fell by an estimated 35%. Nevertheless, malaria remains a major killer of under-fives, claiming the life of 1 child every 2 minutes.
Trends in the scale-up of malaria interventions
Vector control is the main way to prevent and reduce malaria transmission. Two forms of vector control are effective in a wide range of circumstances: insecticide-treated mosquito nets (ITNs) and indoor residual spraying (IRS).
ITNs are the cornerstone of malaria prevention efforts, particularly in sub-Saharan Africa. Over the last 5 years, the use of treated nets in the region has increased significantly: in 2015, an estimated 53% of the population at risk slept under a treated net compared to 30% in 2010.
Indoor residual spraying of insecticides (IRS) is used by national malaria programmes in targeted areas. In 2015, 106 million people globally were protected by IRS, including 49 million people in Africa. The proportion of the population at risk of malaria protected by IRS declined from a peak of 5.7% globally in 2010 to 3.1% in 2015.
Diagnostics
WHO recommends diagnostic testing for all people with suspected malaria before treatment is administered. Rapid diagnostic testing (RDTs), introduced widely over the past decade, has made it easier to swiftly distinguish between malarial and non-malarial fevers, enabling timely and appropriate treatment.
New data presented in the report show that, in 2015, approximately half (51%) of children with a fever who sought care at a public health facility in 22 African countries received a malaria diagnostic test compared to 29% in 2010. Sales of RDTs reported by manufacturers rose from 88 million globally in 2010 to 320 million in 2013, but fell to 270 million in 2015.
Treatment
Artemisinin-based combination therapies (ACTs) are highly effective against P. falciparum, the most prevalent and lethal malaria parasite affecting humans. Globally, the number of ACT treatment courses procured from manufacturers increased from 187 million in 2010 to a peak of 393 million in 2013, but subsequently fell to 311 million in 2015.
Prevention in pregnancy
Malaria infection in pregnancy carries substantial risks for the mother, her fetus and the newborn child. In Africa, the proportion of women who receive intermittent preventive treatment in pregnancy (IPTp) for malaria has been increasing over time, but coverage levels remain below national targets.
IPTp is given to pregnant women at scheduled antenatal care visits after the first trimester. It can prevent maternal death, anaemia and low birth weight, a major cause of infant mortality. Between 2010 and 2015, there was a five-fold increase in the delivery of 3 or more doses of IPTp in 20 of the 36 countries that have adopted WHO’s IPTp policy – from 6% coverage in 2010 to 31% coverage in 2015.
Insecticide and drug resistance
In many countries, progress in malaria control is threatened by the rapid development and spread of antimalarial drug resistance. To date, parasite resistance to artemisinin – the core compound of the best available antimalarial medicines – has been detected in 5 countries of the Greater Mekong subregion.
Mosquito resistance to insecticides is another growing concern. Since 2010, 60 of the 73 countries that monitor insecticide resistance have reported mosquito resistance to at least 1 insecticide class used in nets and indoor spraying; of these, 50 reported resistance to 2 or more insecticide classes.
Progress towards global targets
To address remaining challenges, WHO has developed the Global Technical Strategy for Malaria 2016-2030 (GTS). The Strategy was adopted by the World Health Assembly in May 2015. It provides a technical framework for all endemic countries as they work towards malaria control and elimination.
This Strategy sets ambitious but attainable goals for 2030, with milestones along the way to track progress. The milestones for 2020 include:
Reducing malaria case incidence by at least 40%;
Reducing malaria mortality rates by at least 40%;
Eliminating malaria in at least 10 countries;
Preventing a resurgence of malaria in all countries that are malaria-free.
Progress towards the GTS country elimination milestone is on track: In 2015, 10 countries and areas reported fewer than 150 locally-acquired cases of malaria. A further 9 countries reported between 150 and 1000 cases.
However, progress towards other GTS targets must be accelerated. Less than half (40) of the 91 malaria-endemic countries are on track to meet the GTS milestone of a 40% reduction in malaria case incidence by 2020. Progress has been particularly slow in countries with a high malaria burden.
Forty-nine countries are on track to achieve the milestone of a 40% reduction in malaria mortality; this figure includes 10 countries that reported zero malaria deaths in 2015.
Funding trends
In 2015, malaria funding totalled US$ 2.9 billion, representing only 45% of the GTS funding milestone for 2020. Governments of malaria-endemic countries provided 32% of total funding. The United States of America and the United Kingdom are the largest international funders of malaria control and elimination programmes, contributing 35% and 16% of total funding, respectively. If the 2020 targets of the GTS are to be achieved, total funding must increase substantially.
Cover of World Health Organization’s “World Malaria Report 2015,” which reported dramatic progress controlling malaria.
World Malaria Report 2015 dropped in mid-December, with United Nations-style fanfare.
Which means, you probably heard little to nothing about it in U.S. media, and “conservatives” and anti-science hoaxsters hope you won’t ever see it, so they can claim contrary to the facts that liberals kill kids in Africa.
My cynicism about the fight against malaria dissipates some, but my cynicism about hoaxes substituting for political dialogue grows.
World Health Organization (WHO) releases an annual report near the end of every year, detailing the fight against malaria and progress or lack of it.
Good news this year: WHO estimates deaths to malaria fell below 500,000 per year in 2015. That’s at least a 50% reduction since renewed vigor in the malaria fight in 2000, and it’s a 90% reduction from peak DDT use years, 1958-1963, when WHO estimated 5 million people died each year from malaria.
About 80% of malaria deaths take children under the age of 5.
Bigger picture: Malaria is on the run. Humans are winning the fight against malaria. Much remains to be done, however. Plus, malaria fighters warn that malaria can come roaring back, if governments neglect to follow through on promises of funding, and with well-run programs to cure humans of malaria and prevent new cases.
World Malaria Report 2015 should influence policy discussions in U.S. elections. But generally, this report was ignored.
Millard Fillmore’s Bathtub will feature in-depth discussions of parts of the report, and simple repetition for the record of the report, as part our long-term battle against hoaxsters who claim the U.S. ban on use of DDT on U.S. farms somehow increased malaria in Africa, and killed millions, when malaria actually decreased and millions were saved from death.
Malaria loses only with hard work on the ground by medical people treating and curing humans of the disease, and by public health people working hard to prevent new infections. Most of that work is not glorious, occurs relatively anonymously and away from television cameras and photographers with access to social media. Which is to say, the hard work of defeating malaria goes unsung around the world. We should work to change that.
What did others say about World Malaria Report?
A collection of Tweets, and other links, for your study.
I get e-mail from Texas Gov. Greg Abbott, and all too often it leaves me shaking my head in disgust.
This one came today. I suppose one needs to understand that the e-mail is intended to mislead the recipients about what Gov. Abbott is doing.
In the War on Cancer, Abbott has sided with cancer. As Attorney General in the later stages of the wilting administration of the beleaguered Rick Perry, Abbott refused to investigate a Texas Constitutionally-established, billion-dollar fund to support cancer research whose administration then-Gov. Perry had turned over to old political friends.
Abbott should have recused himself from any investigation by his office, because under the laws setting up the research fund, he was on the board. Any investigation would need to answer the question about what Abbott had done to be sure the funds were spent as the law intended.
Conflicts of interest don’t bother Greg Abbott, though, so long as the conflicts work in favor of his friends, and political donors.
Fortunately for Texas, there is another, separate office to investigate public wrongdoing in state agencies, the Public Integrity Unit of the Travis County District Attorney’s office. That office indicted one of the cancer agency’s officials (he was convicted of misappropriating $11 million in public funds), and promised to indict more.
This so angered Perry he stepped all over the Texas Constitution to bring down the Travis County DA — and that earned Perry his own indictment after an investigation by a GOP-led task force. Oh, yeah, there were other shenanigans by Perry that he might have wanted to cover up; but the cancer research abuse already sent one Perry buddy to jail.
You get the idea. Cancer research is political in Texas, and probably not all that serious a concern to GOP elected officials. Cancer is something poor people get. Republicans have health insurance.
For years, Planned Parenthood clinics in Texas and the rest of the nation offered free cancer screenings and checkups to women who otherwise could not get them for lack of money. These services have nothing to do with abortion, but a lot to do with obstetrical and gynecological care poor women cannot get otherwise.
Read Abbott’s fund-raising letter — yes, he wants me (and you) to donate to his unholy campaign against women’s health care — and pay particular attention to how he avoids any mention of what kinds of services this funding cut-off will kill. He wants you to think he’s fighting abortion.
Which might be oddly and rarely true, if his denial of cancer screenings enables cancer to kill a woman who might have later gotten an abortion, or destroy her ability to conceive at all.
See the letter, sent with the subject, “Another win against Planned Parenthood”:
___________________________________
Friend,
_______________________________________
So there you have it. Greg Abbott wants you to send him money, because he’s stopped poor women in Texas from getting cancer screenings.
Because, abortion, liberty, guns, and probably, illegal immigrants.
And, because he can get away with it.
How stupid must a Texas politician be to think promoting cancer will help any of those problems? How conniving must one be to try to hoodwink Texans into sending him money, neglecting to mention it’s money to support cutting medical care to women who need it?
How stupid must Texas voters be, if they don’t see through this corrupt ruse?
As a journalist, this guy has a piece of a world-wide scoop.
India is probably the last nation on Earth producing DDT. In the last decade other two nations making the stuff got out of the business — North Korea and China. For several years now India has been the largest manufacturer of DDT, and far and away the greatest user, spraying more DDT against malaria-carrying mosquitoes, sand flies, and agricultural and household pests than the rest of the world combined.
As if an omen, India’s malaria rates did not drop, but instead rose, even as malaria rates dropped or plunged in almost every other nation on Earth.
Under the 2001 Stockholm Convention on Persistent Organic Pollutants (POPs) signed by more than 150 nations (not including the U.S.), DDT was one of a dozen chemicals targeted to be phased out due to its extremely dangerous qualities, including long-term persistence in the environment and bioaccummulation, by which doses of the stuff increase up the food chain, delivering crippling and fatal doses to top predators.
A perfect substitute for DDT in fighting some disease-carrying insects (“vectors”) has never been developed. Health officials asked, and the Stockholm negotiators agreed to leave DDT legally available to fight disease. Annex B asked nations to tell the World Health Organization if it wanted to use DDT. Since 2001, as DDT effectiveness was increasingly compromised by resistance evolved in insects, fewer and fewer nations found it useful.
The site Mr. Nazakat linked to is up and down, and my security program occasionally says the site is untrustworthy. It’s obscure at best. Shouldn’t news of this type be in some of India’s biggest newspapers?
I found an article in theDeccan Herald, confirming the report, but again with some
India-United Nations pact to end DDT use by 2020
India-United Nations pact to end DDT use by 2020
New Delhi, August 26, 2015, DHNS:
It would be better to switch to another insecticide, says expert
India is the lone user of DDT, though only in the malaria control programme, while rest of the world got rid of the chemical that has a lasting adverse impact on the environment. DH file photo
India has launched a $53 million project to phase out DDT by 2020 and replace them with Neem-based bio-pesticides that are equally effective.
India is the lone user of DDT, though only in the malaria control programme, while rest of the world got rid of the chemical that has a lasting adverse impact on the environment.
India on Tuesday entered into a $53 million (Rs 350 crore) partnership with the United Nations Industrial Development Organisation (UNIDO), United Nations Environment Programme and the Global Environment Facility to replace DDT with safer, more effective and green alternatives.
“As per the plan, the National Botanical Research Organisation, Lucknow, tied up with a company to produce Neem-based alternatives for the malaria programme. The production will start in six months,” Shakti Dhua, the regional coordinator of UNIDO told Deccan Herald.
Till last year, the annual DDT requirement was about 6,000 tonnes that has now been cut down to 4,000 tonnes as the government decided to stop using it in the Kala-Azar control programme.
A recent study by an Indo-British team of medical researchers found that using DDT without any surveillance is counter-productive as a vector control strategy as sand flies not only thrive but are also becoming resistant to DDT.
“It would be better to switch to another insecticide, which is more likely to give better results than DDT,” said Janet Hemingway, a scientist at the Liverpool School of Tropical Medicine. While the Health Ministry wanted to bring in synthetic pyrethroids, the United Nation agencies supports the bio-pesticides because of their efficacy and long-lasting effects.
“The new initiative would help check the spread of malaria and other vector-borne diseases. These include botanical pesticides, including Neem-based compounds, and long-lasting insecticidal safety nets that will prevent mosquito bites while sleeping,” Dhua said.
Ending the production and use of DDT is a priority for India as it is a signatory to the Stockholm Convention on Persistent Organic Pollutants (POP) of 2002 that seeks to eliminate the use of these chemicals in industrial processes, drugs and pesticides. DDT is one of the POPs.
The clock is counting down the last years of DDT. Good.
If events unroll as planned, DDT making will end by 2020, 81 years after it was discovered to kill bugs, 70 years after it was released for civilian years, 70 years after problems with its use was first reported by the U.S. Fish and Wildlife Service, 58 years after the publication of Rachel Carson’s Silent Spring, 50 years after European nations banned some uses, 48 years after the famous U.S. ban on agricultural use, 19 years after the POPs Treaty.
“End Malaria Now” demonstration from Jolkona.org, Seattle
Remarkable progress against malaria marks the 21st century — but there was even more progress between 1960 and 2000. This progress usually is not noted in screeds against the World Health Organization (WHO), or Rachel Carson, or “crazy environmentalists.”
Through the 1950s, WHO estimated malaria deaths worldwide at about 5 million people each year. In about a decade of WHO’s malaria eradication campaign in temperate zones, the toll is estimated to have dropped to about 4 million dead each year. WHO suspended the eradication campaign in 1963 when it was discovered that mosquitoes in central Africa were already resistant and immune to DDT, which was the chief pesticide used for Indoor Residual Spraying to temporarily knock down local mosquito populations. WHO tried to find substitutes for DDT, but by 1969 formally ended the program and stopped asking for money for eradication.
The fight against malaria continued, however. In 1972 the U.S. flooded malaria-prone nations with DDT which had been intended for use on U.S. crops, after the U.S. prohibited DDT on U.S. crops. For a dozen years all U.S. DDT production got channeled into Africa and Asia to fight disease. U.S. makers had gotten out of DDT production by 1985 as production shifted to other nations.
Despite DDT’s failure, progress was made in medical care and especially in education on how to prevent mosquito bites. The death toll dropped toward 1 million annually until about 1990. In the late 1980s, the medicines used to cure humans from malaria parasites failed, as the parasites developed their own resistance to the drugs. Through the 1990s, malaria deaths remained constant, or even rose.
A flood of concern in the late 1990s produced a coalition of malaria fighters with funding through the United Nations and non-governmental organizations (NGOs) such as the Gates Foundation and Wellcome Trust. In 1999, most of these groups agreed to fight harder, using “integrated vector management,” a variety of methods calculated to prevent mosquitoes from developing resistance to new pesticides, and prevent the malaria parasites from developing resistance to pharmaceuticals.
Plus, in nations where houses often were leaky to mosquitoes, these agencies provided bednets to prevent bites of malaria-carriers at peak biting periods, when people slept. By 2008, deaths dropped below a million each year for the first time, and progress has continued.
Beating malaria is a top goal of the United Nations’ Millennium Development Goals (MDGs); Malaria No More reported on a recently-completed report on those goals, which noted the progress against malaria.
Malaria Deaths Reach All Time Low, U.N. Secretary General’s Final MDG Report Shows
NEW YORK, NY – July 6, 2015 – Malaria deaths have reached an all-time low and 6.2 million lives have been saved from the disease between 2000-2015, according to a new United Nations report announced by U.N. Secretary-General Ban Ki-moon’s office today. The final report on progress of the Millennium Development Goals (MDGs), which are set to expire this year, highlights an historic 69 percent decline in the rate of child deaths from malaria in Africa.
The report provides an update to all eight MDG Goals. The unprecedented global leadership over the past ten years to combat malaria has not only surpassed the disease-specific MDG target (Goal 6, Combat HIV/AIDS, Malaria and Other Diseases), but those efforts also contributed to critical progress toward achieving Goals 4 (Reduce Child Mortality) and 5 (Improve Maternal Health).
“Malaria is one of the standout successes of the MDGs thanks to continuous innovation, bold endemic country leadership and steadfast donor commitment,” said Ray Chambers, the U.N. Secretary-General’s Special Envoy for Malaria and Financing the Health MDGs. “We need to build on this success to ensure no child, woman or man dies from a mosquito bite and that we ultimately eradicate this disease.”
Thanks to the leadership of the United States, the Global Fund to Fight AIDS, Tuberculosis and Malaria and other international donors, malaria financing has grown dramatically from 2000-2015 to more than $3 billion annually, and political leadership has fueled the delivery of more than 1 billion mosquito nets to Africa along with hundreds of millions of effective tests and treatments.
Although these results have successfully surpassed the MDG target, the fight against malaria is not finished. Malaria remains a major global health security challenge with an estimated 3.3 billion people at risk globally. Thanks to recent success in achieving real and measureable progress, coupled with steadfast political leadership and a promising pipeline of transformative new technologies, malaria-affected regions have set ambitious goals for elimination including transformative 2020 targets in Southern Africa, Southeast Asia and the Caribbean.
“Malaria is one of the oldest and deadliest diseases in human history,” said Martin Edlund, CEO of Malaria No More. “For the first time in history we have the opportunity to capitalize on our success and end malaria within a generation; we can’t afford to miss that opportunity.”
Estimated change in malaria incidence rate (cases per 1,000 population at risk) and malaria mortality rate (deaths per 100,000 persons at risk), 2000-2015. USNews.com chart, based on MDG report.
Save
Spread the word; friends don't allow friends to repeat history.
Several good developments in the War on Malaria, worldwide — along with some alarming signs. Maybe there will be time to blog seriously about each of these things later. Let’s get them known, and keep discussion going for the best way to beat malaria in a post-DDT world.
QPharm Tweeted about DSM 265, an experimental, one-dose treatment developed by the Medicines for Malaria Venture (MMV); the video is useful for the background those new to the issue can get on the problems of treating malaria, which make great hurdles for campaigns to eradicate malaria.
In 2013, there was around 584,000 #Malaria related deaths globally. View this video on some amazing work being done https://t.co/mUBleTanJQ
DSM265 is a selective inhibitor of the plasmodial enzyme called DHODH. DHODH is a key enzyme in the replication of the parasite. If we can inhibit that enzyme with DSM265, we can stop the life of the parasite.
Voice of America reported on Rollback Malaria’s call for $100 billion to be spent in the next 15 years, to stamp out the disease.
$100B Plan Seeks to Cut Malaria Cases, Deaths by 90 Percent http://t.co/VmxCPBb8Ff – really important real funding – now what about #EDCTP2?
Malaria deaths are, in 2015, at an “all time low.” Deaths hover around 500,000 per year, most in Africa, and most among children under the age of 5. A staggering total, until compared to the post-World War II estimates of more than 5 million deaths per year, or the more than 3 million deaths per year in 1963, the year the World Health Organization (WHO) had to stop its ambitious campaign to eradicate malaria when pesticide DDT, upon which the campaign was based, produced resistance in mosquitoes in areas where the campaign had not yet reached.
Beating malaria is one of the Millennium Development Goals of the United Nations; this year’s report on MDG acknowledged the great progress already made.
Medical News Now’s Fast Facts on Malaria. Notable, that annual deaths now are way below the million mark. Good news!
One malaria vaccine has won approval for final testing. Good news, though anyone who follows vaccines knows it will take a while to test, and anyone who knows malaria fighting knows there are four different parasites, and delivery of any medical care is tough in far too many parts of the world where any form of malaria is endemic. Even small good news is good news.
Screen capture of the Wellcome Trust HTML presentation on the life cycle of malaria parasites. Malaria fighters know all this almost instinctively; too often policy makers fail to understand it, and so they recommend policies that do not make medical or economic sense in fighting the disease. Click image to go to Wellcome Trust site for full presentation.
Britain’s Wellcome Trust takes as one of its key missions the fight against malaria. The Trust is a charitable foundation created from profits of pharmaceutical development and sales.
Recently I found this HTML animation presentation on the life cycle of the malaria parasite, something all malaria fighters must know to be effective.
It’s also something that DDT advocates seem unable to comprehend. Malaria is not a virus, nor is it a venom mosquitoes manufacture, but it is a parasite that infects (and disables) both mosquitoes and humans. Mosquitoes catch the parasite from an infected human host. After the malaria parasite completes a couple of cycles in the gut of the mosquito, the parasite can be transmitted back to humans by a mosquito bite. And the cycle continues.
Since complete eradication of malaria-carrying mosquitoes is practically impossible in almost all cases, beating malaria requires an interruption in the cycle of transmission of the parasite, plus the curing of the disease in infected human hosts.
For example, the old World Health Organization (WHO) malaria eradication campaign, which operated from 1955 to 1963, DDT was used to temporarily knock down a population of mosquitoes, with hopes human hosts would be ridded of malaria parasites so that, in six months or so, when the mosquito populations roared back, there would be no malaria in local humans to infect mosquitoes. Consequently, mosquitoes can’t transmit a parasite they don’t have.
Lost on far too many people: Humans must be cured of malaria to prevent transmission. Beating malaria takes a lot more than just killing mosquitoes.
U.S. Supreme Court hearing oral arguments in King v. Burwell. The decision issued on June 25, 2015. Image from Newsworks. [Continued search for credit information on this image turned up this caption; artist is Dana Verkouteren of Associated Press] “This courtroom artist rendering shows Michael Carvin, lead attorney for the petitioners, right, speaking before the Supreme Court in March. King v. Burwell, a major test of the Affordable Care Act, could halt health care premium subsidies in all the states where the federal government runs the insurance marketplaces. (AP Photo/Dana Verkouteren)
In all the rending of garments and gnashing of teeth about the Supreme Court’s decision in the Burwell case today, you’d be lucky to learn what the Court actually said.
Here are the key paragraphs of the majority’s decision (links added here), as written by Chief Justice John Roberts:
Reliance on context and structure in statutory interpretation is a “subtle business, calling for great wariness lest what professes to be mere rendering becomes creation and attempted interpretation of legislation becomes legislation itself.” Palmer v. Massachusetts, 308 U. S. 79, 83 (1939). For the reasons we have given, however, such reliance is appropriate in this case, and leads us to conclude that Section 36B allows tax credits for insurance purchased on any Exchange created under the Act. Those credits are necessary for the Federal Exchanges to function like their State Exchange counterparts, and to avoid the type of calamitous result that Congress plainly meant to avoid.
* * *
In a democracy, the power to make the law rests with those chosen by the people. Our role is more confined—“to say what the law is.” Marbury v. Madison, 1 Cranch 137, 177 (1803). That is easier in some cases than in others. But in every case we must respect the role of the Legislature, and take care not to undo what it has done. A fair reading of legislation demands a fair understanding of the legislative plan.
Congress passed the Affordable Care Act to improve health insurance markets, not to destroy them. If at all possible, we must interpret the Act in a way that is consistent with the former, and avoids the latter. Section 36B can fairly be read consistent with what we see as Congress’s plan, and that is the reading we adopt.
The judgment of the United States Court of Appeals for the Fourth Circuit is
Among other goals of the hoaxsters who claim Rachel Carson was wrong and evil, and that the imaginary ban on DDT to fight malaria causes “millions of deaths,” is the erosion of trust in international organizations that lead the fight against malaria, especially WHO, UNICEF and USAID. Sadly, the hoaxsters have friends in Congress who threaten to withhold funding to fight malaria, often insisting that now-mostly-ineffective DDT be used instead of good, working preventive measures and medicines to cure humans of malaria.
And so, Nothing But Nets writes to ask for help:
Dear Ed,
Imagine this: working from 4:00 AM until well into the night, getting very little sleep, traveling along unpaved roads for hours at a time – all to deliver 2,000 bednets per day to the hardest-to-reach children and families.
Email your members of Congress and let them know that you support full funding for malaria prevention programs.
In Mozambique, this is a typical day for health workers as they distribute nets to save lives as part of a campaign funded by the Global Fund to Fight AIDS, Tuberculosis and Malaria. Thanks to the work of the Global Fund and other partners – including UN agencies and local communities on the ground – bednet coverage in Mozambique has gone from less than 5 percent of the population in 2000 to an impressive 60 percent today.
Your member of Congress will vote soon on how much assistance the U.S. will provide to the Global Fund, along with partners like the President’s Malaria Initiative and the United Nations, the core agencies leading the fight against malaria. By showing your support to your representatives in Washington, you can help to make them champions in the fight against malaria and ensure that these bednets continue to make it to families who need them the most.
Or, until that account is unsuspended by the forces supporting Donald Trump: Follow @FillmoreWhite, the account of the Millard Fillmore White House Library
We've been soaking in the Bathtub for several months, long enough that some of the links we've used have gone to the Great Internet in the Sky.
If you find a dead link, please leave a comment to that post, and tell us what link has expired.
Thanks!
Retired teacher of law, economics, history, AP government, psychology and science. Former speechwriter, press guy and legislative aide in U.S. Senate. Former Department of Education. Former airline real estate, telecom towers, Big 6 (that old!) consultant. Lab and field research in air pollution control.
My blog, Millard Fillmore's Bathtub, is a continuing experiment to test how to use blogs to improve and speed up learning processes for students, perhaps by making some of the courses actually interesting. It is a blog for teachers, to see if we can use blogs. It is for people interested in social studies and social studies education, to see if we can learn to get it right. It's a blog for science fans, to promote good science and good science policy. It's a blog for people interested in good government and how to achieve it.
BS in Mass Communication, University of Utah
Graduate study in Rhetoric and Speech Communication, University of Arizona
JD from the National Law Center, George Washington University
 Leave a Comment » |
Leave a Comment » |  History, History of Science, medicine, Science, Vaccinations | Tagged: health, Health care, medicine, Science, Vaccines |
History, History of Science, medicine, Science, Vaccinations | Tagged: health, Health care, medicine, Science, Vaccines |  Permalink
Permalink
 Posted by Ed Darrell
Posted by Ed Darrell 







 _______________________________________
_______________________________________

















