Bedside Communication
Bedside Communication
Download as pptx, pdf, or txt
You might also like
- Clinical Practice Guidelines For The Obstetrician - GynecologistDocument79 pagesClinical Practice Guidelines For The Obstetrician - GynecologistAngela Caguitla67% (3)
- Directions In: PsychiatryDocument44 pagesDirections In: Psychiatrybrad_99100% (2)
- Falls Prevention Program Ipsg: Ahmad ThaninDocument12 pagesFalls Prevention Program Ipsg: Ahmad Thaninmanoj reddyNo ratings yet
- Restraint CompetencyDocument6 pagesRestraint CompetencyFrederick RyanNo ratings yet
- Hsag Qapi CompanionDocument21 pagesHsag Qapi CompanionAngel Inestroza100% (1)
- Day 3 Activity: Nursing Care Plan: College of Health SciencesDocument6 pagesDay 3 Activity: Nursing Care Plan: College of Health SciencesAngelica Charisse BuliganNo ratings yet
- The COAT & Review Approach: How to recognise and manage unwell patientsFrom EverandThe COAT & Review Approach: How to recognise and manage unwell patientsRating: 5 out of 5 stars5/5 (1)
- Mechanical Ventilation For NursingDocument65 pagesMechanical Ventilation For Nursingsasmita nayakNo ratings yet
- 15Document21 pages15Tyson Easo JonesNo ratings yet
- Nursing ManagementDocument11 pagesNursing ManagementAnjelika Eurelle Caliboso MapiliNo ratings yet
- Nursing Documentation, Record Keeping and Written CommunicationDocument14 pagesNursing Documentation, Record Keeping and Written CommunicationAnil Pabba0% (1)
- Assisting in IV TherapyDocument4 pagesAssisting in IV TherapyMaricris Dianne D BondocNo ratings yet
- Fall Risk Care Plan NHS PDFDocument2 pagesFall Risk Care Plan NHS PDFBelayetNo ratings yet
- Information Broucher Nursing ExcellenceDocument16 pagesInformation Broucher Nursing ExcellenceShantu Shirurmath100% (1)
- QI Project On Medication Reconciliation at AdamaDocument9 pagesQI Project On Medication Reconciliation at Adamawassie gebi100% (1)
- Pressure Ulcer Risk Assessment The Braden Scale: Deepesh Bhardwaj Associate ProfessorDocument13 pagesPressure Ulcer Risk Assessment The Braden Scale: Deepesh Bhardwaj Associate ProfessorLaly ThomasNo ratings yet
- Charge NurseDocument2 pagesCharge NurseMes Dela CruzNo ratings yet
- Role of Nurses in Disaster and EmergencyDocument9 pagesRole of Nurses in Disaster and EmergencyS.R.CogoNo ratings yet
- Infection Control Protocols at Travancore Medical College HospitalDocument8 pagesInfection Control Protocols at Travancore Medical College Hospitaltummalapalli venkateswara raoNo ratings yet
- RestraintsDocument16 pagesRestraintsSowjanyaNo ratings yet
- Little Schmidy Falls Risk AssessmentDocument1 pageLittle Schmidy Falls Risk AssessmentrenystrawberryNo ratings yet
- 2012 Stoma and Wound Training PROGRAM - SPMCDocument2 pages2012 Stoma and Wound Training PROGRAM - SPMCHarby Ongbay AbellanosaNo ratings yet
- NE2.1 Ward RoutinesDocument3 pagesNE2.1 Ward RoutinesKatrina PonceNo ratings yet
- Management of Status Asthmatic Us in ChildrenDocument7 pagesManagement of Status Asthmatic Us in Childrenjshq1971No ratings yet
- ICU StaffnurseDocument4 pagesICU StaffnurseMARUTI NURSINGNo ratings yet
- Challenges of Being A Critical Care NurseDocument14 pagesChallenges of Being A Critical Care NurseKatie PurryNo ratings yet
- Job Descriptionof ICNDocument5 pagesJob Descriptionof ICNsari sasiNo ratings yet
- Catheter-Associated Urinary Tract InfectionsDocument20 pagesCatheter-Associated Urinary Tract Infectionsapi-315336673No ratings yet
- He One - Minute Learner Huddle The One-Minute PreceptorDocument3 pagesHe One - Minute Learner Huddle The One-Minute PreceptorScheila MaiNo ratings yet
- Registered Nurse Interview QuestionsDocument5 pagesRegistered Nurse Interview QuestionsahmadNo ratings yet
- Care of Terminal Ill PatientDocument75 pagesCare of Terminal Ill PatientVivek SinghNo ratings yet
- TransitionDocument13 pagesTransitionDonna NituraNo ratings yet
- Guidline of Management of Porta CathDocument8 pagesGuidline of Management of Porta CathroncekeyNo ratings yet
- Nursing Audit (Form)Document16 pagesNursing Audit (Form)jhingjhing09No ratings yet
- Nursing AuditDocument26 pagesNursing AuditpkvNo ratings yet
- GRD Performing Nasopharyngeal Nasotracheal SuctioningDocument2 pagesGRD Performing Nasopharyngeal Nasotracheal SuctioningApril Florendo100% (1)
- Staff Nurse Evaluation FormDocument1 pageStaff Nurse Evaluation FormKrystel Jen AsentistaNo ratings yet
- Rapid Response Team WorksheetDocument1 pageRapid Response Team Worksheetapi-403028741No ratings yet
- Nursing DirectorDocument11 pagesNursing DirectorDimitri EroticoNo ratings yet
- Types of Skin Traction PresentationDocument16 pagesTypes of Skin Traction PresentationZerjohn Seniorom100% (1)
- Blood TransfusionDocument5 pagesBlood TransfusionMoustafa Hazzaa100% (1)
- Nursing AuditDocument21 pagesNursing AuditSam Tully0% (1)
- 6 Steps / Phases OF Nursing ProcessDocument24 pages6 Steps / Phases OF Nursing ProcessMary Anthonette Arenas EstradaNo ratings yet
- NCP 1Document2 pagesNCP 1Roscelie KhoNo ratings yet
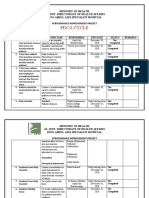
- Pdca CycleDocument4 pagesPdca CycleHamid BouleghabNo ratings yet
- Competencies of Staff EducatorsDocument17 pagesCompetencies of Staff EducatorsCherry Mae L. VillanuevaNo ratings yet
- Blood Transfusion ReactionDocument9 pagesBlood Transfusion ReactionReema Akberali noorani0% (1)
- Chart AuditDocument3 pagesChart AuditAnonymous WJtqIhhvPNo ratings yet
- Multiple Choice Question Acn FinalDocument11 pagesMultiple Choice Question Acn FinalIqra rizwanNo ratings yet
- 2010 Integrated - Updated Circulation ACLS Prehospital Fibrinolytic Checklist PDFDocument1 page2010 Integrated - Updated Circulation ACLS Prehospital Fibrinolytic Checklist PDFms_lezahNo ratings yet
- Vascular Disorder Case StudyDocument3 pagesVascular Disorder Case StudyAaron Wallace100% (1)
- Central Venous CatheterizationDocument34 pagesCentral Venous CatheterizationMujeeb NangrajNo ratings yet
- Skill Laboratory Practice Module: Block: Reproductive System: 10 Topic: Pap SmearDocument5 pagesSkill Laboratory Practice Module: Block: Reproductive System: 10 Topic: Pap SmearMuthiana Rizky0% (1)
- Recovery Room NurseDocument5 pagesRecovery Room NurseChristin 'Kirei' AndoloNo ratings yet
- Checklist On Intravenous Insertion 1.1Document2 pagesChecklist On Intravenous Insertion 1.1Geylla Faeldonia100% (1)
- Suctioning: Prepared By: Christian Ravina M.sc. (N), 2 Year M.T.I.N. ChangaDocument25 pagesSuctioning: Prepared By: Christian Ravina M.sc. (N), 2 Year M.T.I.N. ChangaGrace GurdielNo ratings yet
- Documentation, Nursing Rounds, Manual & ProtocolDocument22 pagesDocumentation, Nursing Rounds, Manual & ProtocolSUNNY__SIJINo ratings yet
- Problem Solving in Nursing Methode 1Document22 pagesProblem Solving in Nursing Methode 1Ina ReginaNo ratings yet
- Modified Early Warning Score (MEWS) Observation Chart: Clinical ProtocolDocument4 pagesModified Early Warning Score (MEWS) Observation Chart: Clinical ProtocolElena DolcanNo ratings yet
- Competences of Advanced NursingDocument8 pagesCompetences of Advanced NursingNatukunda DianahNo ratings yet
- Leaping the Hurdles: The Essential Companion Guide for International Medical Graduates on their Australian JourneyFrom EverandLeaping the Hurdles: The Essential Companion Guide for International Medical Graduates on their Australian JourneyNo ratings yet
- What Is StrokeDocument6 pagesWhat Is StrokeY. Beatrice AbigailNo ratings yet
- Pharmacotherapeutics 1 &2-1Document140 pagesPharmacotherapeutics 1 &2-1Y. Beatrice AbigailNo ratings yet
- Pathophysiology of Burns in DetailDocument46 pagesPathophysiology of Burns in DetailY. Beatrice AbigailNo ratings yet
- Leukemia Cancer of The Blood: Professor Rolland Merch M. Arriza Mindanao State University - General Santos CityDocument31 pagesLeukemia Cancer of The Blood: Professor Rolland Merch M. Arriza Mindanao State University - General Santos CityY. Beatrice AbigailNo ratings yet
- Recent Advances in The Management of BurnsDocument11 pagesRecent Advances in The Management of BurnsY. Beatrice AbigailNo ratings yet
- Pathophysiology of Burns - 1Document32 pagesPathophysiology of Burns - 1Y. Beatrice Abigail50% (2)
- Disorders of Accesssory Organs in GI SystemDocument29 pagesDisorders of Accesssory Organs in GI SystemY. Beatrice AbigailNo ratings yet
- Management of Patients With Gastro-Intestinal DisordersDocument84 pagesManagement of Patients With Gastro-Intestinal DisordersY. Beatrice AbigailNo ratings yet
- DIABETESDocument43 pagesDIABETESY. Beatrice AbigailNo ratings yet
- 1) Nursing Careplan For FeverDocument9 pages1) Nursing Careplan For FeverY. Beatrice AbigailNo ratings yet
- Multiple Choice Questions (GIT)Document4 pagesMultiple Choice Questions (GIT)Ahmed AliNo ratings yet
- Model Question Paper HDT BP603TDocument3 pagesModel Question Paper HDT BP603Tmohdajaj1999No ratings yet
- RabeprazoleDocument7 pagesRabeprazoleعبدالمحسن علي ENo ratings yet
- P S L Gy: Posology and Dosage RegimenDocument7 pagesP S L Gy: Posology and Dosage RegimenRaj Kumar SoniNo ratings yet
- Homeosiniatry - Combination of Acupuncture and HomeopathyDocument4 pagesHomeosiniatry - Combination of Acupuncture and HomeopathyGold Sunrise100% (1)
- Surgery Cases: CASE 2: Chest Abdominal TraumaDocument3 pagesSurgery Cases: CASE 2: Chest Abdominal TraumaGio Tamaño BalisiNo ratings yet
- Patient Information SheetDocument2 pagesPatient Information SheetDavis JermacansNo ratings yet
- Passmedicine Mcqs-resp & EntDocument63 pagesPassmedicine Mcqs-resp & Entsiddiq SiddiquiNo ratings yet
- TOG Volume 26 Issue 4Document51 pagesTOG Volume 26 Issue 4bdeekshithgouda92No ratings yet
- Breast CA ScreeningDocument8 pagesBreast CA Screeningchristelm_1No ratings yet
- Summary Basic Life Support (PBL 7) .Document2 pagesSummary Basic Life Support (PBL 7) .Youssef Mansour100% (1)
- Fourth Year MCQ in Psychiatry 2011 PDFDocument19 pagesFourth Year MCQ in Psychiatry 2011 PDFSpacetoon DaysNo ratings yet
- 3.clostridium TetaniDocument15 pages3.clostridium TetaniPravesh NiraulaNo ratings yet
- Parenteral Medication - PPT 1Document78 pagesParenteral Medication - PPT 1Tatah Rasma A. Hadjali100% (1)
- Obtaining A Capillary Blood Specimen To Measure Blood GlucoseDocument3 pagesObtaining A Capillary Blood Specimen To Measure Blood GlucoseFranz Earl Niño AlbesaNo ratings yet
- Alcoholic Liver DiseaseDocument70 pagesAlcoholic Liver Diseaseaannaass nNo ratings yet
- Download ebooks file Fundamentals of Skeletal Radiology 5th Edition Clyde A. Helm all chaptersDocument21 pagesDownload ebooks file Fundamentals of Skeletal Radiology 5th Edition Clyde A. Helm all chapterszlocksikka9l100% (2)
- Herpes Simplex KeratitisDocument20 pagesHerpes Simplex KeratitisriskhapangestikaNo ratings yet
- Activity-2.2-STNationBldg - (Scientist) GUINEADocument2 pagesActivity-2.2-STNationBldg - (Scientist) GUINEAKiethNo ratings yet
- Reconstructive Aesthetic Implant SurgeryDocument156 pagesReconstructive Aesthetic Implant SurgeryOanaroxana Varsa100% (2)
- Assessing The Utility of ChatGPT Throughout The Entire Clinical WorkflowDocument15 pagesAssessing The Utility of ChatGPT Throughout The Entire Clinical Workflowbeatzmine20No ratings yet
- IFU - Exdia CRP - Rev.00 PDFDocument2 pagesIFU - Exdia CRP - Rev.00 PDFДаниил АртеменкоNo ratings yet
- VA Statement On Nelson's AppointmentDocument2 pagesVA Statement On Nelson's AppointmentcronkitenewsNo ratings yet
- Hypertension in The Young AgesDocument1 pageHypertension in The Young AgesYai MeiNo ratings yet
- NeuroDocument4 pagesNeuroKrizia R. PingkeNo ratings yet
- Clinical Practice Guidelines For Physical Therapy in Patients With Intermittent ClaudicationDocument51 pagesClinical Practice Guidelines For Physical Therapy in Patients With Intermittent ClaudicationsilkofosNo ratings yet
- Anambra State College of Health Technology 000Document2 pagesAnambra State College of Health Technology 000Philip EzechukwuNo ratings yet