Long term
care
purpose
To identify chronically ill and functionally disabled elders for whom the
provision of care and
expanded services results in reduced use of currently covered nursing
home, acute medical, or home
health services.
To improve the care, reduce mortality, morbidity, and improve
satisfaction with care, and other
potential measures of quality enhancements resulting from long-term
care.
The resident shall provide appropriate assessment to facilitate early
intervention and treatment
measures when serious medical condition presents.
definition
Long-term care provides services that assist a member with assistance
with walking, bathing,
dressing, feeding, toileting, and supervision of medication that can
normally be self-administered.
Services should be provided by qualified, trained and registered
healthcare team.
Assessment: systemic collection and review of patient data collected
through patient focused
observations, interviews, measurements and diagnostic tests.
Reassessment: continuous process of data gathering to determine
significant changes or the
continuance if needs.
policy
The patient's medical and nursing needs shall be identified from the initial assessments, which
should
be completed and documented in the patient health record.
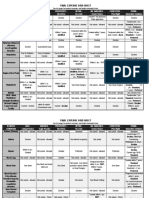
Assessment data includes biophysical, psychological, functional, nutritional, educational and social
data:
Biophysical - review of relevant major body systems and appropriate psychological
parameters, including pain.
Psychological - initial interpretation as to how the patient perceives this healthcare encounter,
e.g. noncompliance to offered treatment, suspected drug abuse, emotional / behavioral
problems, etc.
Functional assessment of ability to perform activities of daily living including Patient ability
to position himself/herself in bed, restricted Range of Movements (ROM), Change in Muscle
Power, Impaired Daily Living Activities.
Nutritional relevant dietary information about nutritional screening and assessment Criteria to
identify malnourished patients, assignment of appropriate malnutrition Risk levels, development of
nutrition intervention plan, and performance of nutrition Reassessment based on the
malnutrition risk
level at defined time interval such as D.M, Poor Appetite more than 3 days, Tube feeding, Food
allergy, difficulty in swallowing / chewing, Psychological eating disorder, patient in critical care
units, overweight, sudden change in weight, major surgery, hyperemesis gravidarum, diarrhea
more
than 4 days, palliative care, needs therapeutic diet.
Educational and learning needs, including determination of family/ community support and
supplies
required after discharge from the hospital.
Social-Economic - relevant information about support systems in the home situations and
spiritual,
economic/financial factors, cultural factors, Emotional, social, psychological factors, non-
compliance
to treatment Physical/mental disabilities e.g. Living alone, suspected abuse or neglect, cultural
or
religious background that would need to know for the plan of care, unable to assess due to lack
of
procedure
. Assessment:
4.1.1. Initial assessment (upon admission):
[Link]. Past medical and surgical history
[Link]. Current medical issues.
[Link]. Functional status/ Mobility limitations
[Link]. Family support
[Link]. Recent changes in mental status
[Link]. History of depression or anxiety
[Link]. Signs of abuse
4.1.2. Identify risk for:
[Link]. Falls
[Link]. Loss of Skin integrity
[Link]. Sensory problem (e.g. Visual, auditory)
4.1.3. Assess mental status on admission and daily for:
[Link]. Orientation
[Link]. Ability to follow simple commands
[Link]. Restlessness
[Link]. Lethargy.
Assess vital signs on admission
Weigh, Height and BMI
Assess the following physical parameters:
Signs of dehydration or fluid overload (e.g. peripheral edema, dry
mucous membranes, altered mental status, crackles in lung fields).
Intake (food and fluids) and behavioral patterns associated with eating,
drinking or swallowing (e.g. choking, wet voice quality after taking
liquids,pocketing/pouching food in cheek, watery eyes and difficulty
swallowing). Note: evaluate need for aspiration precautions.
Continence (e.g. frequency of urination, use of bedpan or toilet, bowel
routine including consistency and frequency of stools)
Sensory impairment in hearing, vision and/or balance that
can affect function ,such as need for hearing aids, contact lenses,
glasses or assistive device such as cane or walker.
Assess the following behavioral parameters:
Thought problems (e.g. disorganized thought, sad affects,
depression, and changes in interactions with staff or family
members).
Sleep patterns (e.g. naps in daytime, number of hours sleep
at night and bedtime habits).
Pain expression: evaluate need for pain management.
Identify and respect the patient’s personal and environmental
boundaries considering culture, sensory challenges and
psychosocial independence.
Care Partner:
Identify the care partner that will be primary responsible to take
care of patient after discharge.
Care:
Discuss the plan of care with patient and the care partner.
Encourage patient or caregiver’s active participation in activities
of daily living, evaluate need for occupational therapy/physiotherapy
consultation
Encourage independence as much as applicable.
4.4. Reassessment:
4.4.1. Daily reassessment should be conducted and include revision of all points assessed at
admission in addition to the below:
[Link]. Pain score;
[Link]. Last vital signs (BP, pulse, respiration, temperature);
[Link]. Time of last medication(s); and
[Link]. Patient/Family preferences for care
4.5. Activities of Daily Living
4.5.1. Assist with personal hygiene, hand washing before eating and after toileting.
4.5.2. Promote balance of rest and activity to preserve energy (e.g. limit night time awakening.
4.5.3. Ensure that all prosthetics are utilized to maximize patient’s participation. Maximize
patient’s ability to transfer/ambulate by:
[Link]. Maintaining head of bed in upright position (90-degree angle) to patient’s
tolerance at least 2 minutes before patient stands/transfers
[Link]. Observe signs of postural changes (dizziness, unsteadiness, reports of feeling
weak/faint cheek lying, standing BP/Heart rate if this is observed)
Nutrition/Fluid Balance
Identify food preferences4
Assure patient is properly positioned to reduce risk of aspiration
Wear dentures if appropriate
Sit upright in bed or chair with chin tucked in
Provide slow unhurried pace
Remain in upright position for 30 minutes after eating
Offer fluids of choice every two hours to drink independently
Initiate referral to dietician for consideration of alternative nutritional
supplements if taking
<50 % of diet
4.7. Elimination:
4.7.1. Assist patient to toilet/bedside commode.
4.7.2. Avoid use of diapers as it encourages incontinence and reduce self-esteem.
4.7.3. Avoid use of indwelling catheters.
4.7.4. Record intake/output every shift.
4.8. Cognitive/Sensory:
4.8.1. Consider effects of medication, infections, dehydration, pain and need to void
as potential sources of confusion.
4.8.2. Optimize communication by using the following techniques with patient:
[Link]. Use a quiet soothing voice
[Link]. Use one-step instructions
[Link]. Be consistent when giving instructions and providing care
[Link]. Avoid arguing with patient
4.8.3. Anticipate needs which the patient may be unable to express (e.g. hunger,
thirst, toileting, position change, pain).
4.8.4. Adjust environment to accommodate auditory and visual deficits.
Avoid over stimulation:
Keep light low
Use soothing music
Decrease activity around patient
Avoid using TV for diversion
Monitor frequently when confused and re-orient as needed.
Alert to time of day
Modify environment to assure patient safety:
Arrange furniture so pathway to bathroom is free of barriers
Maintain low light at night
Keep assistive devices within reach
Lock wheels on all rolling furniture
Emphasize need to stabilize and prevent further deterioration.
Teach patient/caregiver measures to promote safe environment
Discuss with patient/caregiver how to communicate needs to health care
providers.
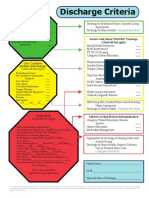
Discharge planning should begin at time of admission for patients typically include the following
elements:
Demographics;
Primary language;
Family members/notification of discharge;
Primary diagnoses;
Allergies;
Medications (including immunizations and reconciliation review);
Diet
Advance directives;
Mental status;
History of falls;
Skin integrity;
Assistive/protective devices (i.e., hearing aids, glasses, walkers, etc.)
ADL status;
Special instructions;
Belongings sent; and
Follow up care.
REFERENCES:
10.1. Lee CH, Cheng CL, Chang CH, et al. Universal pharmacological thromboprophylaxis
for total knee
arthroplasty may not be necessary in low-risk populations: a nationwide study in Taiwan.
J Thromb
Haemost 2012; 10:56.
10.2. Zareba P, Wu C, Agzarian J, et al. Meta-analysis of Randomized Trials Comparing
Combined
Compression and Anticoagulation with either modality alone for prevention of venous
thromboembolism after surgery. Br J Surg 2014; 101:1053.
10.3. VTE Guideline, King Fahad Medical City-Riyadh, Ministry of Health-KSA.
10.4. Sachdeva A, Dalton M, Amaragiri SV, Lees T. Graduated compression stockings for
prevention of
DVT. Cochrane Database Syst Rev 2014; 12:CD001484.
11