ACNE
Uploaded by
2226205ACNE
Uploaded by
2226205First-, second-, and third-line therapies should be appropriate for the
severity and staging of the clinical presentation and directed toward control
113 and prevention.
Treatment regimens should be tapered over time, adjusting to response.
Acne Vulgaris Combine the smallest number of agents at the lowest possible dosages to
ensure efficacy, safety, avoidance of resistance, and patient adherence.
Debra Sibbald Once control is achieved, maintenance regimens should be simplified to
continue with some suppressive therapy. Therapy must be continued
beyond 8 weeks: efficacy is assessed through comedonal and inflammatory
KEY CONCEPTS lesion count, control or progression of severity, and management of
associated anxiety or depression. Safety end points include monitoring for
Acne is a highly prevalent disorder affecting adolescents and adults, with a
treatment adverse effects.
large psychosocial impact.
Motivate the patient to continue long-term therapy through empathic and
The etiology of this complex disease originates from multiple causative and
informative counseling.
contributory factors, including genetics and environment. The diagnosis is
based on the patient’s history and clinical presentation.
Acne is a disease of the pilosebaceous unit. Elements of pathogenesis
involve defects in epidermal keratinization, androgen secretion, sebaceous Preclass Engaged Learning Activity
function, bacterial growth, inflammation, and immunity.
Watch the video entitled “Acne” by Dr Sheilagh Maguiness, pediatric
Acne vulgaris is a chronic disorder which cannot be “cured.” Goals of dermatologist, available on the Society for Pediatric Dermatology Website
treatment and prevention include control and alleviation of symptoms by ([Link] This 5-minute video provides a brief overview
reducing the number and severity of lesions, slowing progression, limiting regarding information patients need to know about acne vulgaris. The video is
disease duration and recurrence, prevention of long-term disfigurement useful to enhance student understanding regarding what information to
associated with scarring and hyperpigmentation and avoidance of provide to patients regarding causes of acne, triggers, cleansing, over the
psychologic suffering. Targeting goals may increase patient adherence to counter and prescription options, directions for use and precautions. It gives a
therapy. brief summary of take-home points useful to direct counseling.
The most critical target for treatment is the microcomdedone. Minimizing
or reversing follicular occlusion will arrest the pathogenic acne cascade and
involve combining treatment measures to target all pathogenic elements. INTRODUCTION
Nondrug measures are aimed at long-term prevention and treatment.
In this chapter, I review the latest developments in understanding acne vulgaris
Patients should eliminate aggravating factors, maintain a balanced, low-
and its treatment. The contents provide an analysis of the physiology of the
glycemic load diet, and control stress. Cleanse twice daily with mild soap
pilosebaceous unit; the epidemiology, etiology, and pathophysiology of acne;
or soapless cleanser and use only oil-free cosmetics. Comedone extraction
relevant treatment with nondrug measures; and comparisons of pharmacologic
in approximately 10% of patients produces immediate cosmetic
agents, including drugs of choice recommended in best-practice guidelines.
improvement. Shave infrequently as possible, using a sharp blade or
Options include a variety of alternatives such as retinoids, antimicrobial agents,
electric razor.
hormones, and light therapy. Formulation principles are discussed in relation to
drug delivery. Patient assessment, general approaches to individualized therapy perception that acne is less prevalent in rural populations. This is supported by
plans, and monitoring evaluation strategies are presented. the data from Varanasi, India, where 21.35% of boys (13-18 years) from rural
areas had acne versus 37.5% of those from the urban areas.7
EPIDEMIOLOGY An international group of epidemiologists, community medicine specialists,
and anthropologists have questioned whether acne might be predominantly a
Acne vulgaris is a chronic disease and the most common one treated by disease of Western civilization.8 They assert that since acne vulgaris is nearly
dermatologists. There is a high degree of variability in prevalence, age of onset, universal in westernized societies (afflicting 79%-95% of the adolescent
distribution, severity, and age of resolution. population), one causative factor might be the Western glycemic diet. While this
The lifetime prevalence of acne approaches 90%, with the highest incidence hypothesis is based on the observation that primitive societies subsisting on
in adolescents. Prevalence data available from the European Union, United traditional (low glycemic) diets have no acne, the theory awaits validation and
States, Australia, and New Zealand show that acne affects 80% of individuals acceptance by the dermatologic community.
between puberty and 30 years of age, depending on the method of lesion
counting (50%-95% prevalence range reported for adolescents and 20%-30% ETIOLOGY
prevalence range for ages 20-40).1 Other studies have reported acne in 28% to
61% of school children aged 10 to 12 years; 79% to 95% of those 16 to 18 years Acne is a multifactorial disease. Genetic, racial, hormonal, dietary, and
of age; and even in children aged 4 to 7 years. If mild manifestations were environmental factors have been implicated in its development. Its psychologic
excluded and only moderate or severe manifestations were considered, the impact can be severe.
frequency in epidemiological studies in Western industrialized countries was still Four major etiologic factors are involved in the development of acne:
20% to 35%.2–5 increased sebum production, due to hormonal influences; alteration in the
The onset of acne vulgaris during puberty occurs at a younger chronologic keratinization process and hyperproliferation of ductal epidermis; bacterial
age in girls than boys (12% age 25-58 vs 3% in males of the same age) and colonization of the duct with Propionibacterium acnes; and production of
periodic premenstrual flares may continue until menopause. It is triggered in inflammation with release of inflammatory mediators in acne sites. These are
children by the initiation of androgen production by the adrenal glands and reviewed in the Pathophysiology section later in this chapter.
gonads, and it usually subsides after the end of growth. However, to some The role of heredity in acne has not been clearly defined; however, there is a
degree, most patients continue to have symptoms into their mid-twenties, and significant tendency toward more serious involvement if one or both parents had
there is evidence that the duration of acne may last into middle age for most severe acne during their youth.
women, recorded in 54% of women and 40% of men older than 25 years of age.6 Environmental factors play a major role in determining the severity and
In puberty, acne is often more severe in boys in about 15% of cases, which is 10- extent of acne and may influence the choice of topical treatments. Heat and
fold greater than in girls. Women often have more severe forms during humidity may induce comedones; pressure or friction caused by protective
adulthood. When untreated, acne usually lasts for several years until it devices such as helmets, shoulder pads, or pillows, and excessive scrubbing or
spontaneously remits. After the disease has ended, scars and dyspigmentation are washing can exacerbate existing acne by causing microcomedones to rupture.
not uncommon permanent negative outcomes. Pressure may cause acne lesions to form in patients who do not have acne
Genetic factors have been recognized; there is a high concordance among vulgaris: this variant is called mechanical acne. Friction, wool, or other rough
identical twins, and there is also a tendency toward severe acne in patients with a textured fabrics and occlusive clothing may also be mechanical irritants. Hair
positive family history of acne. styles that are low on the forehead or neck may cause excessive sweating and
There are believed to be no gender differences in acne prevalence, although occlusion, exacerbating acne. In most cases acne is worse in winter and
such differences are often reported and may represent social biases. In urban improves during the summer, suggesting a salutary effect of sunlight. However,
clinics, there is a clear preponderance of girls seeking treatment. There is also a in some cases, exposure to sunlight worsens the disease.9 Studies examining the
relationship between tobacco smoking and acne show inconsistent results; controlled trial, patients who eliminated high glycemic index foods showed a
however, dermatologists have begun to counsel people to quit tobacco smoking significant reduction in acne. Those who consumed a low-glycemic-load diet
as a potential auxiliary treatment for acne. compared with a conventional HGL diet had improvements of facial acne after
The importance of psychologic factors in this prolonged and capricious 12 weeks. Accompanying changes in physical and endocrinologic parameters
condition has been repeatedly stressed. Two-thirds of affected teenagers wish suggest that decreases in total energy intake, body weight, and indices of
that they could speak with their physician and healthcare provider about acne, androgenicity and insulin resistance may also be associated with observed
but only one-third do. Emotions, such as intense anger and stress, can exacerbate improvements in acne.23 Another study reported an improvement in acne and
acne, causing flares or increasing mechanical manipulation: picking, excoriating, insulin sensitivity in low-glycemic-load diets compared with controls,
or pinching lesions sometimes subconsciously or in sleep. This is probably the suggesting nutrition-related lifestyle factors play a role in acne etiology.24
result of increased glucocorticoid secretion by the adrenal glands, which appears Independent effects of weight loss versus dietary intervention need to be
to potentiate the effects of androgens.10 isolated. In an Australian study, participants who consumed low glycemic load
Dietary influences Current investigations explore associations between diets had no reported cases of acne.17
dietary influences and acne. Under study are dietary influences as factors in acne Other studies showed correlations between increases in the ratio of saturated
development as well as potential treatment modalities. This follows the dismissal to monounsaturated fatty acids, acne lesion counts and increased sebum outflow,
of over-interpreted 40-year-old, poorly designed studies that disavowed potential suggesting a possible role of desaturase enzymes in sebaceous lipogenesis and
effects of dietary ingestions on acne.11–14 Three primary influences on the clinical manifestation of acne. These require further investigation.25
development include dairy and growth factors in milk; whey protein in milk; and Univariate and multivariate analyses were used to examine results of a 2015
hyperglycemic-load diets. French survey of individuals (age 15-24 years) reporting or not reporting acne
A series of studies have linked consumption of dairy products with acne.15,16 with associated epidemiologic variables. Daily consumption of chocolate and
Acne has been positively associated with the reported quantity of milk ingested, sweets (odds ratio 2.38) and regular use of cannabis (odds ratio 2.88) was
particularly skim milk.17 The Nurses Health Retrospective Study examining diet independently and highly associated with acne. Smoking tobacco (>10 cigarettes
during high school in 47,355 women found an association between acne and daily) was highly protective. Respective roles of sugar, lipids, and milk were not
milk intake, suggesting natural hormonal components of milk and/or other investigated.26
bioactive molecules in milk could exacerbate acne.18 The role of dietary factors in the development or progression of acne vulgaris
Lactoferrin is a whey milk protein with anti-inflammatory activity. cannot be dismissed. Currently, practical recommendations would be to avoid
Lactoferrin-enriched fermented milk ameliorated acne vulgaris, selectively excess sugar and skim milk. Further studies are ongoing, including reviewing
decreasing triacylglycerols in skin surface lipids.18 Lactoferrin administered as a antioxidants from nutritional and topical sources and probiotics as potential
dietary supplement twice daily in mild-to-moderate acne vulgaris led to an acne-fighting agents.17
overall improvement in acne lesion counts in adolescents and young adults.19
A recent meta-analysis of observational studies examined association of dairy PATHOPHYSIOLOGY
intake and acne in children, adolescents, and young adults. Any dairy product—
including milk, yogurt, and cheese—was associated with an increased odds ratio The pathogenesis of acne includes hyperseborrhea, abnormal follicular
for acne in individuals aged 7 to 30 years; however, studies were heterogenous in keratinization, and Propionibacterium acnes proliferation in the pilosebaceous
design, making comparisons difficult.20 unit. Recent research has shed some new light on the involvement of the
Other studies suggest a role for insulin-like growth factor (IGF), increased by sebaceous gland, as well as on the pro-inflammatory activity of the cutaneous
ingestion of high glycemic loads.21,22 The strongest evidence supports a high microbiome. Acne progresses through the following four major stages:
glycemic load (HGL) diet as a significant factor in acne. In a randomized 1. Increased sebum production by the sebaceous gland
2. P. acnes follicular colonization (and bacterial lipolysis of sebum
triglycerides to free fatty acids)
3. Release of inflammatory mediators
4. Increased follicular keratinization
Improved understanding of acne development on a molecular level suggests that
acne is a disease that involves both innate and adaptive immune systems and
inflammatory events. Receptors that regulate sebaceous lipid metabolism work
in concert with receptors regulating epidermal growth and differentiation. Acne
can be considered as a model of immune-mediated chronic inflammatory skin
disease: an innate immune response that is not able to control P. acnes followed
by a Th1-mediated adaptive immune response that becomes self-maintaining
independently from P. acnes itself.27
Acne usually begins in the prepubertal period, when the adrenal glands
mature, and progresses as androgen production and sebaceous gland activity
increase with gonad development. During puberty, alteration of the sebaceous
lipid profile, called dysseborrhoea, together with stress, irritation, cosmetics, and
potential dietary factors lead to inflammation and formation of different types of
acne lesions.28
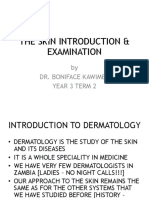
As shown in Fig. 113-1, acne results from the development of an obstructed
sebaceous follicle, called a microcomedone. Sebaceous glands increase their size
and activity in response to circulating androgens. Most patients with acne do not
overproduce androgens (with some exceptions); instead, they have sebaceous
glands that are hyperresponsive to androgens.29 Patients with acne have a FIGURE 113-1 Cascade of the pathogenesis of acne. (Reprinted with
significantly greater number of lobules per gland compared with unaffected permission from Mills OH, Kligman AM. Comedogenicity of sunscreens:
individuals. experimental observations in rabbits. Arch Dermatol 1982;18(6):417-419.)
Sebum production is induced by different receptors expressed by the
sebaceous gland. Involved are the histamine receptor (activated by histamines),
the hormonal DHT receptor, (activated by androgens); the neuromodulator
receptor (mainly substance P); and corticotrophin-releasing hormone (CRH)
receptor (mainly activated by stress); recent molecular research has identified
three other receptors that are expressed by the sebocyte and control sebum
production. Each of these newly identified receptors is activated by a dietary
substance.28
The peroxisome proliferator-activated receptors are stimulated by free fatty
acids and cholesterol, which act in concert with retinoid X receptors to regulate
epidermal growth and differentiation as well as lipid metabolism.
The insulin-like growth factor (IGF)-1 receptor is stimulated by sugar to As the plug extends to the upper canal and dilates its opening, an open
increase lipid formation, mediated by sterol response element binding proteins. comedone, or blackhead, is formed. Its dark color is not due to dirt but to either
The leptin receptor is stimulated by fat. Leptin is responsible for creating lipid oxidized lipid and melanin or to the impacted mass of horny cells. The
droplets within the sebocyte and induces pro-inflammatory enzyme and cytokine cylindrically shaped, open comedone is very stable and may persist for a long
(interleukin (IL)-6 and IL-8) secretion as well.28 time as soluble substances and liquid sebum escape more easily. Acne that is
The sebaceous gland also acts as an endocrine organ in response to changes in characterized by open and closed comedones is termed noninflammatory acne.
androgens and other hormones. Oxidized squalene can stimulate Acne produces chemotactic factors and promotes the synthesis of tumor
hyperproliferative behavior of keratinocytes, and lipoperoxides produce factor-α and interleukin-1β. Cytokine induction by P. acnes occurs. Both
leukotriene B4, a powerful chemoattractant.29 The composition of sebum is recruitment of polymorphs into the follicle during the inflammatory process and
changed, with a reduction in linoleic acid. The growth of keratinocytes changes. release of P. acnes–generated chemokines lead to pus formation. The pus
The infrainfundibulum increases its keratinization of cells with eventually bursts on the surface with resolution of the inflammation or into the
hypercornification and development of the microcomedone, the primary lesion dermis. P. acnes also produces enzymes that increase the permeability of the
of both noninflammatory and inflammatory acne.27 Cells adhere to each other in follicular wall, causing it to rupture, releasing keratin, hair, and lipids and
an expanding mass, which forms a dense keratinous plug. Androgen hormones irritating free fatty acids into the dermis. Several different types of inflammatory
could be a stimulus to pilosebaceous duct hypercornification. Sebum, produced lesions may form, including pustules, nodules, and cysts and may lead to
in increasing amounts by the active gland, becomes trapped behind the keratin scarring.
plug and solidifies, contributing to open or closed comedone formation. Postinflammatory hyperpigmentation (PIH) and scarring are two sequelae of
Interleukin-1-α upregulation contributes to the development of comedones acne. A time delay of up to 3 years between acne onset and adequate treatment
independently of colonization with P. acnes. A relative linoleic acid deficiency correlates to degree of scarring and emphasizes the need for early therapy.11,12
has also been described.29
A prominent role is played by the follicular colonization by P. acnes. P. acnes CLINICAL PRESENTATION
displays several activities which promote the development of acne lesions,
including the promotion of follicular hyperkeratinization; the induction of To correctly diagnose acne vulgaris, the clinician considers patient assessment,
sebogenesis; and the stimulation of an inflammatory response by the secretion of which includes distinguishing all the presenting signs and symptoms of the
proinflammatory molecules and by the activation of innate immunity, followed clinical presentation, reviewing diagnostic and assessment considerations (see
by a P. acnes-specific adaptive immune response. In addition, P. acnes- Clinical Presentation box), as well as considering psychosocial issues,
independent inflammation mediated by androgens or by a neurogenic activation, differential diagnosis, and the possibility of drug-induced acne.
followed by the secretion in the skin of proinflammatory neuropeptides, can
occur in acne lesions.27
Psychosocial Issues
The pooling of sebum in the follicle provides ideal substrate conditions for
proliferation of the anaerobic bacterium P. acnes, generating a T-cell response, Acne causes profound negative psychological and social effects on the quality of
which results in inflammation.30 P. acnes produces a lipase that hydrolyzes life (QOL) of patients. Assessment of acne’s impact on QOL is an important
sebum triglycerides into free fatty acids. These free fatty acids may trigger the consideration in clinical decision-making. The negative impact of facial acne is
changes that lead to an increase in keratinization and microcomedone one of the primary motivators for patients to seek and to adhere to treatment.40
formation.31,32 This closed comedone, or whitehead, is the first clinically visible The European Dermatology Forum S3-Guideline for the Treatment of Acne
lesion of acne. It takes approximately 5 months to develop. The closed recommended adopting a QOL measure as an integral part of acne
comedone is almost completely obstructed to drainage and has a tendency to management.41 Specific QOL indicators represent patients’ perceptions of and
rupture.33–35 reactions to their health. Assessing QOL impairment in patients with acne may
aid in management by evaluating psychologic impact, which may not correlate Differential Diagnosis
with clinical severity; aid in detection of depression or need for psychologic
care; and improve therapeutic outcomes. Acne vulgaris is rarely misdiagnosed. The conditions most commonly mistaken
Acne adversely affects all aspects of QOL. In addition to documentation for acne vulgaris include rosacea, perioral dermatitis, gram-negative folliculitis,
regarding acne-specific QOL impairment, acne impact on general health and and drug-induced acne.48
psychologic status has been assessed for relationship between sociodemographic Acne rosacea (adult acne) is a chronic, progressive relapsing condition
variables, disease severity, and mental status on QOL of acne sufferers. In a occurring after age of 30 years in fair-complexioned persons. The diagnosis is
report of 195 cases, acne impact on health status was worse compared to other clinical and based on history and physical findings. There are four subtypes:
chronic diseases. Authors concluded acne is not a minor disease in comparison erythemato-telangietactic changes (erythema, flushing, telangiectasia [spider
with other chronic conditions. Age of onset is capable to influence general health veins], stinging and burning); progressing to papular-pustular changes
quality (GHQ status), which in turn affects QOL.42 Patients with acne (inflammatory lesions, with edema, papules, and pustules on central facial areas
experience functioning and emotional effects from their skin disease comparable such as nose, cheeks, chin, and forehead); phymatous changes (thickened skin
with those experienced by patients with psoriasis, and patients with severe acne and prominent pores on nose, ears, chin, and eyelids; and ocular changes
reported levels of social, psychological, and emotional problems as great as (foreign body sensation, dryness, burning, eyelid erythema).
those reported by patients with chronic disabling asthma, epilepsy, diabetes, back Rosacea has key differences from acne vulgaris. Onset is not linked to
pain or arthritis.41 androgens or endocrine changes; and comedones are not usually present.
The European Academy of Dermatology and Venereology Task Force on Aggravating factors include endogenous triggers: ingestion of alcohol, spicy
QOL and Patient Oriented Outcomes and the Task Force on Acne, Rosacea and foods, or hot drinks (especially those containing caffeine), smoking; and
Hidradenitis Suppurativa have documented the QOL instruments that have been exogenous triggers: overexposure to sunlight; exposure to temperature extremes,
used in acne patients, with information on validation, purposes of their usage, heat and humidity, friction, irritating cosmetics, and steroids. Treatment may
description of common limitations and mistakes in their usage and overall include antibiotics, particularly doxycycline (low, anti-inflammatory dose) or
erythromycin, topical metronidazole, pimecrolimus or azelaic acid as well as
recommendations.41
agents to reduce erythema (alpha adrenergics).49
There are many global scales that have been used to evaluate acne. Some
Perioral dermatitis occurs primarily in young women and adolescents and is
include the World Health Organization Quality of Life (WHOQOL), Skindex,43
characterized by erythema, scaling, and papulopustular lesions commonly
the Dermatology QOL Index,44 and the Children’s Dermatology Life Quality
clustered around the nasolabial folds, mouth, and chin. The cause is unknown.50
Index (CDLQI). Examples of acne-specific scales include the Acne-specific
Gram-negative folliculitis (Proteus, Pseudomonas, Klebsiella) may
QOL questionnaire,45 the Acne QOL Scale,46 the Acne Disability Index (ADI),
complicate acne, with a sudden change to pustules or large inflammatory cysts
and the Cardiff Acne Disability Index (CADI).41 The Acne QOL Scale was
occurring after long-term treatment of acne with oral antibiotics. Folliculitis may
developed to measure the impact of facial acne across four domains (acne be caused by staphylococci. There is a sudden onset of superficial pustules
symptoms, role-emotional, self-perception, and role-social) of health-related around the nose, chin, and cheeks. Patients with suspected folliculitis should be
QOL. Health-state utilities (such as time trade-off [TTO]) are quantitative
referred.51
measures of patient preferences of health outcomes ranging from 0 (death) to 1
(perfect health) and can be used in clinical trials as outcome measures of Several conditions include acne vulgaris as a characteristic component, and
treatment effects. TTO utilities for acne in the range of 0.94 to 0.96 can be understanding the mechanisms involved in these syndromes provides insight into
compared with those of other diseases (eg, 0.92 for epilepsy, 0.94 for myopia), the pathogenesis of acne. These include polycystic ovary syndrome (elevated
and help to identify the impact of acne on self-perception and psychologic androgen levels); PAPA syndrome (pyogenic arthritis, pyoderma gangrenosum,
acne; early onset arthritis with increased inflammatory activity), and SAPHO
functioning.47
syndrome (synovitis, acne, pustulosis, hyperostosis, osteitis syndrome; sterile
inflammatory arthro-osteitis, with P. acnes as a possible trigger).30 • Pustules and cysts often rupture spontaneously and drain a purulent or
bloody but odorless discharge36
CLINICAL PRESENTATION Acne Vulgaris • Inflammatory lesions may itch as they erupt and can be tender or
painful. Nodules may develop exudative sinus tracts resulting in tissue
Lesion Type: Acne Vulgaris Can Be Noninflammatory or destruction
Inflammatory • Often resolution of these lesions leaves erythematous or pigmented
• Noninflammatory acne is characterized by open and closed comedones macules that can persist for months or longer, especially in dark-
that develop from the subclinical microcomedo skinned individuals
• The closed comedo is visible as a 1-2 mm whitehead most easily seen • Nodules and deep lesions may result in scarring
when the skin is stretched. It is often inconspicuous with no visible
follicular opening.
Regions of Involvement
• Is the first clinical sign of acne • Acne lesions can occur anywhere on the body apart from the palms and
soles
• Has a tendency to rupture
• Are usually located on the face, back, neck, shoulders, and chest
• The open comedo or blackhead is large, approximately 2-5 mm, and
dark-topped with contents extruding • May extend to buttocks or extremities
• is relatively stable • One or more anatomic areas may be involved in any given patient
• Inflammatory acne is traditionally characterized as having • The pattern of involvement, once present, tends to remain constant
papulopustular and/or nodular lesions, which may arise from the • Comedones frequently have a midfacial distribution in childhood and,
microcomedo or from noninflammatory clinically apparent lesions when evident early, are indicative of a poor prognosis
• A pustule is formed from a superficial aggregation of neutrophils. • Skin, scalp, and hair are frequently oily
• Appears as a raised white lesion filled with pus, usually less than 5
mm in diameter Severity Grading Taxonomies
• Superficial pustules usually resolve within a few days without scarring US Food and Drug Administration (FDA) Investigator Global Assessment
200537,38
• A nodule is produced through deeper, dermal, inflammatory infiltration
• Is the most severe variant of acne Almost clear: rare noninflammatory lesions with no more
Type 1
• Appears as warm, tender, firm lesions, with a diameter of 5 mm or than 1 small IL
greater Mild, some noninflammatory lesions, no more than a few
Type 2
• May be suppurative or hemorrhagic within the dermis, may involve inflammatory lesions (papules/pustules only, no nodules)
adjacent follicles and sometimes extend down to fat Moderate: many noninflammatory lesions, some
Type 3
• Cysts are suppurative nodules named because they resemble inflamed inflammatory lesions, no more than one nodule
epidermal cysts Severe: up to many noninflammatory and inflammatory
Type 4
• Cystic acne may show double comedones, resulting from prior lesions, but no more than a few nodular lesions
inflammation and fistulous links between neighboring sebaceous units
European Union Guidelines Clinical Classification29,39
• Progression of inflammatory lesions
I Comedonal acne (phenytoin), cyclosporine, and azathioprine. Drugs that most commonly induce
II Mild-to-moderate papulopustular (MMPP) acne papular–pustular reactions include anti-inflammatory medications (NSAIDs),
sulfamethoxazole–trimethoprim, cephalosporins, and diltiazem.
Severe papulopustular acne, moderate nodular acne (this level
III Systemic corticosteroids can cause a pustular inflammatory form of acne,
combines FDA types 3 and 4, above)
especially on the trunk. Onset is abrupt at 2 to 6 weeks after initiation of therapy.
Severe nodular acne, conglobate acne (this is an additional
IV Acne has also been associated with most of the potent topical steroids, but not
level beyond the FDA types above)
with hydrocortisone, which lacks the ability to inhibit protein synthesis.
Discontinuation of the steroid results in an initial worsening of appearance due
Diagnostic and Assessment Considerations
to removal of the anti-inflammatory action of the steroid itself. Caution patients
Palliating factors Sunlight about this reaction, which can be subdued through judicious use of topical
Premenstrual flares, humid environments, excessive hydrocortisone.50–53
sweating; exposure to chemicals; occlusive clothing; Antiepileptics and tuberculostatics are the most commonly implicated in
Provoking factors
friction; oily cosmetics; manual manipulation; stress; drug-induced acne, followed by lithium. Other heavy metals inducing acne
diet (high glycemic load, dairy) include cobalt (in vitamin B12).54 Halogens, especially an excess of iodide in
Associated symptoms Itch, pain, fever seafood, salt, and health foods, can exacerbate acne. In addition, halogens can
May contribute to or coexist with acne, including provoke de novo acne lesions in individuals who have increased external
Medical conditions endocrine factors (eg, irregular menses, hirsutism, exposure often due to occupational contact, or pool or hot tub disinfection; this
alopecia), pregnancy, atopy variant is called chloracne.
May cause acne symptoms, or present a In addition, certain minor ingredients in cosmetics have been implicated in
Allergies
contraindication to therapy cosmetic acne, including isopropyl myristate, cocoa butter, and fatty acids.
Products may cause or interact with acne signs and
Medication history
symptoms TREATMENT
Social habits Diet or smoking
The first step in determining a safe and efficacious treatment regimen for acne
Family history Genetic predisposition to acne vulgaris is to establish desired outcomes for the patient, regarding both short-
Assess global and disease specific quality of life and long-term goals.
Psychosocial issues
(QOL) indicators or health-state utilities
Desired Outcomes (Goals of Treatment)
Acne vulgaris is treated as a chronic disease, as it demonstrates typical
Drug-Induced Acne chronicity characteristics: manifests as either acute outbreaks or slow onset;
In addition to the conditions induced by drugs that are presented in Chapter patterns of recurrence or relapse; a prolonged course; and psychologic and social
e117, “Drug-Induced Dermatologic Disorders,” acneiform eruptions can also be impact. There are two governing principles: the chronic nature warrants early
caused by medications. Drug-induced acne is monomorphic, either comedonal and aggressive treatment, and maintenance therapy is often needed for optimal
with some inflammation or papular–pustular. Drugs most commonly implicated outcomes.
in inducing comedonal/inflammatory acne include those with hormonal effects Acne requires long-term control. This must be stressed with the patient to
(steroids, OCP), halogens (iodide, bromide), vitamins (B2, B6, B12), encourage adherence to lengthy treatment regimens, which address management
tuberculostatic drugs (isoniazid, ethambutol), lithium salts, antiepileptics of current symptoms and signs and preventive measures.
Basic goals of treatment include alleviation of symptoms by reducing the individual spots. Most cause initial skin irritation, which may result in
number and severity of lesions (objective and subjective grading) and improving nonadherence or discontinuation. Irritation can be minimized by starting with
appearance, slowing progression, limiting duration and recurrence, prevention of lower strengths and gradually increasing frequency or dose. Where irritation
long-term disfigurement associated with scarring and hyperpigmentation, and persists, changing formulation from alcoholic solutions to washes, gels, or more
avoidance of psychologic suffering. moisturizing creams or lotions might help.
A significant percentage change in lesion counts is desirable: most patients First-line, second-line, and third-line therapies should be selected and
empirically validate a margin of 10% to 15% reduction in facial lesion counts as altered as appropriate for the severity and staging of the clinical presentation.
appropriate. Patient global self-assessment of acne improvement is a primary Treatment is directed at control, not cure. Regimens should be tapered over time,
outcome. adjusting to response. Combine the smallest number of agents at the lowest
possible dosages to ensure efficacy, safety, avoidance of resistance, and patient
General Approach to Treatment adherence. Once control is achieved, simplify the regimen but continue with
some suppressive therapy. As it takes 8 weeks for a microcomedone to mature,
The most critical treatment target is the microcomedone. Eliminating therapy must be continued beyond this duration to assess efficacy.52 With the
follicular occlusion will arrest the whole acne cascade. Nondrug and exception of topical antibiotics, most topical preparations may be used for years
pharmacologic treatment and preventive measures should be directed toward as needed.
cleansing, reducing triggers, and combination therapy targeting all four Lesions typically recur for years. Microcomedones significantly decrease
pathogenic mechanisms. Combination therapy is often more effective than single during therapy but rebound almost immediately after therapy is discontinued.
therapy and may decrease side effects and minimize resistance or tolerance to The strategy for treating acne includes an induction phase followed by a
individual treatments. maintenance phase, further supported by adjunctive treatments and/or cosmetic
The approach to acne management is largely determined by: routines. Routine maintenance therapy involves regular use of appropriate agents
to ensure remission and reduce potential for recurrence of visible lesions.
1. Severity index For successful long-term treatment, maintenance therapy must be tolerable,
2. Lesion type: predominantly noninflammatory or inflammatory appropriate for the patient’s lifestyle and convenience, continuing months to
3. Treatment preferences including patient choices years, depending on age. Education about pathophysiology of acne and the
4. Cost implications psychosocial benefits of clearer skin are compelling reasons for patient
5. Skin type and/or ethnic group adherence to consistent therapy to sustain remission.
6. Patient age
7. Adherence Nonpharmacologic Therapy
8. Response to previous therapy Encourage patients with acne to discontinue or avoid aggravating factors,
9. Presence of scarring including occlusion from mechanical factors or cosmetics, maintain a balanced,
10. Psychologic effects low-glycemic-load diet, and control stress. Evidence shows that by being
11. Family history of persistent acne empathic and informative during counseling, the health professional may
motivate the patient to continue long-term therapy.8,9,49 One of the first
Topical therapy is the standard of care for mild-to-moderate acne. Those with approaches to nondrug management of acne is attention to cleansing techniques.
moderate-to-severe acne will require systemic therapy. Shaving recommendations, comedone extraction, dietary considerations, issues
Topical treatments work only where applied. To reduce new lesion relating to ultraviolet light, and prevention of cosmetic acne should be reviewed
development, they must be applied to the entire affected area rather than with patients.
• Inhaled systemic or contact allergies to drugs, cosmetics, foods, vehicle
ingredients or excipients
• Objective data
Fitzpatrick phototype
Labs if relevant to monitoring for hepatic or renal function
Assess
• Presence of provoking factors or contributing factors (see Clinical
Presentation/Diagnostic and Assessment Considerations) (eg, hormonal or
adrenal anomalies: presence of vellus hair on females; in children: early
age of onset [age 1-7 years], body odor, hair in axillary and public areas
and adrenal: rapid growth in children)
• Severity: number, type, and region of lesions; presence of scarring
• Hyperpigmentation of healed lesions (postinflammatory
hyperpigmentation)
• Ability/willingness to adhere to long-term therapy
• Emotional status (eg, presence of anxiety, depression)
Plan*
Patient Care Process for Acne Vulgaris • Goals: clear existing and prevent new lesions; reduce scarring,
hyperpigmentation, and psychological impact
Collect • Discontinuation of provoking habits, botanicals or drug or nondrug
• Patient characteristics (eg, age, race, sex, weight [body mass index], measures
pregnant) • Cleansing routine
• Patient medical history (personal and family history, especially of acne or • Drug therapy regimen including dietary, nonpharmacologic and
scarring, adrenal abnormalities) pharmacologic approaches
• Social history (eg, psychosocial issues) and dietary habits including intake • Monitoring parameters including efficacy (eg, improvement or resolution
of glycemic foods, dairy, and sugary drinks (see Clinical of lesions and time frame) and safety (eg, sign and symptoms worsening,
Presentation/Diagnostic and Assessment Considerations; also section irritation, or allergy); frequency and timing of follow-up
“Etiology”)
• Patient education (eg, purpose of treatment, dietary and lifestyle
• Current medications including OTC drug and nondrug measures, modification, drug-specific information, medication administration or
prescription drugs (eg, contraceptives) sunscreens, herbal products, dietary application technique)
supplements, and prior acne medication use
• Self-monitoring for resolution of acne symptoms, occurrence of scarring,
• Current cosmetic use, including makeup, coverups, and cleansers when to seek emergency medical attention
• Current use of devices (eg, comedone extractors)
• Referrals to other providers when appropriate (eg, behavioral health, Soapless cleansers are an alternative to soaps.57 Soaps are the most widely
dietitian) used cleansing products, but do not lend themselves to efficient delivery of
active drug. Two main disadvantages exist. As soaps are rinsed off, the deposit
Implement* of active agent is limited, and the high pH required in soaps may degrade some
• Provide patient education regarding all elements of treatment plan active ingredients and be less tolerable on sensitive skin. Soaps produce a drying
• Use motivational interviewing and coaching strategies to maximize effect on the skin due to detergent action. As medicated cleansers require
adherence increased contact time, this drying action is pronounced, especially with peeling
agents.
• Schedule follow-up, adherence assessment
Gentle liquid cleansers often contain surfactant systems to remove dirt,
Follow-up: Monitor and Evaluate sebum, bacteria, and corneocytes from the skin surface. Oil is dispersed from the
• Improvement or resolution of acne symptoms (eg, noninflammatory or skin into the surfactant system; however, the active ingredient is sometimes
inflammatory lesions) trapped and removed upon rinsing. The balance between cleanliness and drying
or irritation should also be considered. Most patients prefer products with
• Prevention of complications (eg, scarring, infection) foaming action, and these must contain additional secondary surfactants to
• Slow progression enhance the foam and condition the skin.
• Presence of adverse effects There is no evidence that any particular washing regimen is superior.
• Patient adherence to treatment plan using multiple sources of information Evidence-based studies on the use of cleanser or medicated cleansers are lacking
or poorly designed with small numbers of patients.56 It is also difficult to
• Reevaluate duration of therapy every 3 months
compare studies of different nonprescription formulations even when the same
*Collaborate with patient, caregivers, and other healthcare professionals. active ingredient is used, as differences in the composition of vehicle may affect
cutaneous penetration and vehicles themselves may affect acne. Avoid cream-
based cleansers. Scrubbing should be minimized to prevent follicular rupture.
Cleansing Because the acid pH of skin has an antimicrobial effect, it has been proposed
A systematic review of clinical evidence for washing and cleansers reported that that lowering lesional surface pH (with products such as Herpifix, marketed in
they are common interventions. Cleansers are indicated in all patients with acne. Europe) may be correlated to the number of acne lesions. Studies are planned.
However, the clinical evidence for their efficacy is not well understood.55 Synthetic polyester cleansing sponges abrade the skin surface, removing
Twice-daily face washing may be superior to either once-daily or more superficial debris. Considering the structure of comedones, they are unlikely to
frequent washing. Washing too frequently in an attempt to remove surface oils unseat these lesions. Sponges are available in soft or coarse textures, with or
has shown no added benefit and is not likely helpful, as surface lipids do not without soap. Circular or rubbing motions will increase irritation. Instruct
affect acne. Contributory lipids are deep in the follicle and are not removed patients to use single, gentle, continuous strokes on each side of the face, from
through washing. Antiseptic cleansers, while producing a clean, refreshed the midline out toward the ears.
feeling, remove only surface dirt, oil, and aerobic bacteria. They do not affect P. Cationic-bond strips are activated by water. As the strip dries, the cation
acnes. Patients should wash no more than twice daily with a mild, nonfragranced bonds with the anionic dirt and oil in the pores and removes it when the strip is
opaque or glycerin soap or a soapless cleanser. peeled off.
Bar soaps are subclassified into true soaps, comprising an alkali and a fatty
acid, syndet bars, which use synthetic surfactants, and combars, which include Shaving
features of both. A study has suggested syndet bars may be superior to true soaps
Boys and men with acne should try electric and safety razors to determine which
as an acne vulgaris cleansing agent.56
is more comfortable for shaving. When using a safety razor, the beard should be
softened with soap and warm water or shaving gel. Shaving should be done as Prevention of Cosmetic Acne
lightly and infrequently as possible, using a sharp blade and being careful to
avoid nicking lesions. Strokes should be in the direction of hair growth, shaving Persistent low-grade acne is frequently caused by heavy cosmetic use in women
each area only once, to minimize irritation. after their mid-twenties. Adolescent acne in younger women may be exacerbated
with makeup overuse. The problem is perpetuated when resultant blemishes are
Comedone Extraction concealed with more cosmetics.
Patients should be advised to discontinue oil-containing cosmetics and avoid
Comedone extraction has not been widely tested in clinical trials despite long- cosmetic multistep regimens applying various cream-based cleansers and cover-
standing clinical use; however, it is painless and results in immediate cosmetic ups. These are commercially advertised and often available with promotional
improvement. Pretreatment with a peeler for 4 to 6 weeks often facilitates the bonuses through Internet shopping. Three-step basic systems usually combine
procedure.53 Following cleansing with hot water, a comedone extractor is placed medicated and nonmedicated ingredients. The product names used in marketing
over the lesion and gentle pressure applied until the contents are expressed. This these preparations may not make apparent the inclusion of therapeutic agents.
removes unsightly lesions, preventing progression to inflammation. A correctly Initial steps usually involve cleansers, in lotions or creams, which may contain a
sized extractor allows the central keratin plug to extrude through the opening. multitude of unnecessary ingredients, including medicated peelers, oils,
The small end of a plastic eye dropper, with bulb removed, may also be used. fragrances, and preservatives. Active ingredients including salicylic acid, sulfur,
These instruments should be cleaned with alcohol after each use. Some initial or benzoyl peroxide are often included in subtherapeutic or low doses. The
reddening may be apparent. If the contents are not expressed with modest second step is generally a water- or alcohol-based “toner” or “refresher,” which
pressure, patients should not continue since improper extraction may further might contain medicated mild comedolytic agents such as α-hydroxy acids (eg,
irritate the skin. A physician should be consulted if this technique is too difficult glycolic acid), or even a humectant such as glycerin. The final product, often
for the patient to manage. Since the follicle is difficult to remove completely, called intensive or repairing solutions, usually contains the lowest strength of
comedones may recur between 25 and 50 days following expression. Fewer than peelers such as benzoyl peroxide, sulfur, or salicylic acid; plus potentially
10% of comedone extractions are a complete success, but the process is useful sensitizing fragrances and preservatives; or oil-soluble sunscreens not identified
when done properly.36 on the label. Bases may have significant oil content. There may be additional
Comedo removal may be helpful in the management of comedones resistant products such as masks or spot treatments that supplement the base routine of
to other therapies. While the procedure cannot affect the clinical course of the three steps. Multiple-step cosmetic programs are often costly and should be
disease, it can improve the patient’s appearance, which may encourage avoided in favor of simple cleansers and more effective single-ingredient peelers
adherence with the treatment program. at optimal concentrations.
The term noncomedogenic may refer to either water-based vehicles or
Ultraviolet Light products that are free of substances known to induce comedones. They are not
Although ultraviolet light was recommended in the past for desquamation, the necessarily oil-free. Water-based cosmetics may contain significant amounts of
practice is no longer advisable because of the well-established carcinogenic and oil in the form of undiluted vegetable oils, lanolin, fatty acid esters (butyl
photoaging effects of ultraviolet exposure. Moreover, inflamed skin is more stearate, isopropyl myristate), fatty acids (stearic acid), fatty acid alcohols, cocoa
susceptible to the damaging effects of ultraviolet light. Patients taking tretinoin butter, coconut oil, red veterinary petrolatum, and sunscreens containing
may show heightened sensitivity.58 benzophenones. Water-based products are more likely to contribute to pore
Before exposure to sunlight, patients with acne should apply sunscreens (sun blockage than oil-free products.
protection factor [SPF] 15) in alcohol- or oil-free bases and avoid using the Oil-free makeups are well-tolerated and lipstick, eye shadow, eyeliner,
acnegenic benzophenones. Sunscreen should be applied as the first product. eyebrow pencils, and loose face powders are relatively innocuous. Heavier, oil-
based preparations, particularly moisturizers and hairsprays, clog pores and
accelerate comedone formation.59
Patients should restrict cosmetic use including makeup, moisturizers, or stability should be maximized while addressing technical and commercial
sunscreens to products labeled oil-free rather than water-based. Cover-up factors.
cosmetics for acne are available in several skin tones and in lotion and cream Immiscible liquids might be delivered in oil-in-water or water-in-oil
forms. They often contain peeling agents, antibacterial agents, or hydroquinone. emulsions. In addition to having undesirable oil content, these vehicles also
Most contain sulfur. They may be applied as cosmetics two or three times daily, contain humectants, thickeners, preservatives, and fragrance, all of which may
over the entire face or to individual lesions. Because the spread time of oil-free be problematic.
makeup is decreased, best results are achieved if applied to one-quarter of the Solutions are simpler formulations. They are often used as the soaking liquid
face at a time. Topical medication should be applied after gentle cleansing and a for fibrous cloth wipe products. The shelf-life depends upon whether multiple
foundation lotion may be used sparingly as a concealer.60–62 wipe packages are resealable, and whether the solvent volatility will affect
Because the action of most therapeutic acne agents is to dry the skin, the use storage and active agent availability or cause crystallization. Solutions are used
of nonspecific moisturizers is counterproductive. Active agents, such as α- mainly with topical antibiotics, which are often dissolved in specific types of
hydroxy acids (glycolic, lactic, pyruvic, and citric acids), may be present in a alcohol. Although some antibiotics are only soluble in ethyl alcohol, isopropyl
cosmetic formulation, since they reduce corneocyte adhesion.63 Patients with alcohol is generally better able to remove oil from the skin surface and is
acne should be restricted to oil-free α-hydroxy acid products unless necessary preferred for nonmedicated vehicles. Solutions and washes can be more easily
because of treatment with strong drying agents or isotretinoin. applied to large areas such as the back.66
Cosmetics, if correctly prescribed, may improve the performance of the Nongreasy solutions, gels, lotions, and creams should be selected as bases for
therapy, whereas incorrect procedures and/or inadequate cosmetics may worsen topical acne preparations. Lotions and creams will contain some oil-phase
acne. Clinicians should make informed decisions about the role of various ingredients. Discourage moisturizers and oil-based products. Lotions are slightly
cosmetics and to identify the appropriate indications and precautions. The choice less drying than gels, and creams are more emollient. Gels are very useful as
of the most effective product should take into consideration the ongoing they are mixtures of water or alcohol and totally oil free. Many gels contain
pharmacologic therapy and acne type/severity as well.64 ethanol or isopropyl alcohol. Propylene glycol is sometimes present in small
amounts to add viscosity and lessen the drying effects of strong peeling agents.
Vehicles Gels are drying but may cause a burning irritation in some patients and may
Topical medication is a staple in treating mild-to-moderate acne because it is an prevent certain kinds of cosmetics from adhering to the skin.59 Propylene glycol
efficient way to deliver medication to the site of action and involves decreased gels are easy to apply and dry without a visible or sticky film. Nonalcoholic gels
risk of exposure to ingredients. Since local irritation from the vehicle can lead to may be so effective and less drying than alcoholic solutions. Alcoholic or
poor adherence and outcomes, it is essential to choose a vehicle which is acetone gels are usually more drying and provide better penetration of the active
effective and well tolerated. Topical agents are absorbed primarily through ingredient.
passive diffusion via appendageal transcellular or intracellular pathways. As the Consider the patient’s skin type and preferences in the choice of vehicle for
active drug travels, it may undergo chemical changes in the skin or by the topical agents. Patients with oily skin often prefer vehicles with higher
vehicle.65 proportions of alcohol (solutions and gels), while those with dry or sensitive skin
prefer nonirritating lotions and creams. Hydrating and emollient products are
The formulation of an acne vehicle must consider the technical characteristics
often recommended to patients using drying treatment therapies, such as
of maintaining and delivering the drug in an active state together with the need
isotretinoin, to control adverse effects and improve adherence to treatment.
for an elegant product that is well tolerated and the patient will enjoy using, so
Lotions can be used with any skin type and can be easily spread over hair-
that it is more likely to be applied as required and deliver the full benefit.
bearing skin, but they will cause burning or dryness if they contain propylene
Physically and chemically, the vehicle will be used with one or more of the
glycol. Compatibility of vehicles and agents with cosmetics should also be
following goals: reduce excess oil, control bacteria associated with acne, reduce
considered.
the effects of hyperkeratinization, and unclog pores. Performance, safety, and
The focus of innovation has been optimal formulations of problematic drugs. pigmentation, and sebum casual level. Less ultraviolet B light reaches the skin
A fixed topical alcohol-free aqueous gel combination of clindamycin phosphate surface with the hydrocolloid dressing in place.71,72
1.2% and tretinoin 0.025% given once daily simplifies administration and
encourages adherence. Creamy wash and gel hydrophase options for benzoyl
peroxide reduce the irritation of this drug.67 Pharmacologic Therapy
The importance of vehicle effects in topical therapy has been demonstrated in Successful pharmacologic therapy must address one of the four mechanisms
placebo effect literature.67 The percent contribution of vehicle (placebo) toward involved in the pathogenesis of acne. Numerous agents are available that prove
efficacy of reduction of lesions counts of eight commonly prescribed topical one or more of these actions and are therefore effective. However, the choice of
preparations at the end of 10 to 12 weeks of daily administration has been active pharmacologic therapy depends on severity.
reported as a mean value of 55% (range 35%-82%). Mechanisms of drug action relating to acne pathogenesis are illustrated in
Fig. 113-2.
How to Use Topical Preparations
Topical preparations should not be applied to individual lesions but to the whole
area affected by acne to prevent new lesions from developing. Care should be
advised in applying around the eyelid, mouth, and neck (to avoid chafing).
Lotions should be applied with a cotton swab once or twice a day after washing
or at bedtime if they leave a visible residue. Skincare products may cause skin
dryness and redness particularly at the early stages of the treatment. Should this
occur, the product should be applied more infrequently, the treatment should be
stopped for a while or another topical product tried. To reduce irritation a topical
vehicle with high water content may be applied over the medicinal product after
a few minutes; the irritation usually subsides as the skin becomes accustomed to
the topical skincare product.
Psychologic Approaches, Hypnosis, and Biofeedback
The psychologic effects of acne may be profound. The American Academy of
Dermatology expert workgroup unanimously concluded that effective acne
treatment can improve the emotional outlook of patients.68 There is weak FIGURE 113-2 Acne pathogenesis and drug mechanisms.
evidence of the possible benefit of biofeedback-assisted relaxation and cognitive
imagery.69,70
Drug Treatments of First Choice
Dressings There is concordance among key opinion leaders in different settings regarding
recommendations for drugs of choice for management of acne—the Global
A pilot double-blind, randomized study of 20 patients has shown some benefit of
Alliance 2018 and the 2016 European Guidelines.29,39,73
treatment with a hydrocolloid acne dressing when compared with tape dressings
for improving mild-to-moderate inflammatory acne vulgaris. Results showed
greater reduction over 3 to 7 days in the overall severity of acne and Managing Acne
inflammation, along with greater improvement in redness, oiliness, dark For comedonal, noninflammatory acne Active agents of first choice include
those that correct the defect in keratinization by producing exfoliation most recommendation).29,39 As alternative agents, a retinoid fixed combination or oral
efficaciously. Topical retinoids, in particular, adapalene, or a fixed combination antibiotics can be recommended. For females, oral isotretinoin plus
with a retinoid (eg, adapalene plus benzoyl peroxide) can be recommended as antiandrogenic hormonal therapy is preferred. Alternatively a fixed combination
drugs of choice.29,39 Benzoyl peroxide or azelaic acid or salicylic acid can be retinoid with oral antibiotics (consider high dose) and/or oral antiandrogenic
considered, as alternatives (lower strength recommendation).29,39 Limitations hormonal therapy can be recommended.74
can apply that may necessitate the use of a treatment with a lower strength of For maintenance therapy for acne The most frequently recommended
recommendation as a first-line therapy (eg, financial resources and agents are topical retinoids or retinoid and benzoyl peroxide fixed dose
reimbursement limitations, legal restrictions, availability, drug licensing). combinations.73 The most extensively studied maintenance treatment (four
Because the comedone is the initial lesion even in inflammatory acne, these controlled trials) has been adapalene regimens.29,39 Other published options
agents are used to correct the defect in keratinization in all cases of acne. include tazarotene or tretinoin. In general, maintenance therapy is begun after a
For mild-to-moderate papulopustular inflammatory acne It is important 12-week induction and continues for 3 to 4 months. Continuing improvement
to reduce the population of P. acnes in the follicle and the generation of its using this schema is achieved, with relapse occurring when patients stop
extracellular products and inflammatory effects. Either the fixed-dose treatment, suggesting a longer duration of maintenance therapy is likely to be
combination (adapalene and benzoyl peroxide) or benzoyl peroxide or topical beneficial. Topical azelaic acid is an alternative to topical retinoids for acne
retinoid or azelaic acid are strongly recommended as first choice therapy (high maintenance therapy, with advantageous efficacy and safety profiles for long-
strength recommendation).29,39,73 In case of more widespread disease, for the term therapy. To minimize antibiotic resistance, long-term therapy with
treatment of moderate papulopustular inflammatory acne, the fixed-dose antibiotics is not recommended as an alternative to topical retinoids. If an
combination is preferred, with or without hormonal therapy and/or antibiotic, antimicrobial effect is desired, the addition of benzoyl peroxide to topical
particularly if the trunk is involved.73 retinoid therapy is preferred.
Low-strength recommendations are offered as considerations for treatment in
the event of limitations that apply in selecting a first-choice agent. The choices Published Guidelines
would be blue light monotherapy, alternate combination therapy (such as fixed- In general, recommendations should be based on critical appraisal and
dose combination of erythromycin and tretinoin, fixed-dose combination of interpretation of the literature combined with clinical experience. There is
isotretinoin and erythromycin) or oral zinc. In case of more widespread disease, considerable heterogeneity in the acne literature. The large number of products
a combination of a systemic antibiotic with either benzoyl peroxide or with and product combinations, and the scarcity of comparative studies, has led to
adapalene in fixed combination with benzoyl peroxide can be considered.29,39 disparate opinions and few recommendations are evidence-based. Various
For moderately severe or severe papulopustular or moderate nodular evidence-based guidelines, available from multiple American, Canadian,
acne The fixed-dose combination with an oral antibiotic is preferred. European, Scandinavian, and South African sources from 2005 to 2018, do not
Alternatively, oral isotretinoin or oral hormonal therapy can also be added.74 In provide concordance or clarity on all issues.
the event of limitations to use of these agents, considerations could be given to The 2016 European Guidelines for the Treatment of Acne focus primarily on
oral antiandrogens in combination with oral antibiotics or topical treatments, or major treatments, but do not review general management issues such as
systemic antibiotics in combination with benzoyl peroxide (low strength psychologic determinants, scarring, diet, and so forth.29,75 Where relevant,
recommendation). specific information from multiple sources will be integrated into the therapy
section that follows.
Managing Very Severe Acne An expert committee of the American Academy of Dermatology redefined
For nodular or conglobate acne In males, monotherapy with oral isotretinoin is guidelines for acne therapy in 2016 (Table 113-1).74 These guidelines address
strongly recommended as the drug of first choice (high strength the management of adolescent and adult patients presenting with acne but not the
consequences of disease, including the scarring, postinflammatory erythema, or
postinflammatory hyperpigmentation. In 2009, the Global Alliance to Improve
Outcomes in Acne updated their 2003 recommendations to review new
information about pathophysiology and treatment and included current published
data on relevant issues.76 In 2018, the Global Alliance published a further update
providing relevant clinical guidance to healthcare practitioners managing
patients with acne, with an emphasis on areas where the evidence base may be
sparse or needs interpretation for daily practice. They provided 10 consensus
recommendations, based on the 2016 American Academy and European
Guidelines.73
TABLE 113-1 Evidence Chart for Recommendations for Managing Acne
Vulgaris
Complementary and Alternative Medications People with acne often turn to
The Alliance recommendations statements were as follows73: complementary and alternative medicine (CAM), such as herbal medicine,
1. Retinoids have an essential role in treatment of acne. For most patients with acupuncture, and dietary modifications, because of their concerns about the
inflammatory acne, comedonal acne, or both, a topical retinoid plus benzoyl adverse effects of conventional medicines. Although these products might be
peroxide is first-line therapy.29,74,75 well tolerated, very limited data exist regarding their safety and efficacy.
2. The role of antibiotics in acne therapy has changed. Neither topical nor A systematic review of CAM treatments for acne in 2006 identified 15
systemic antibiotics should be used as monotherapy for acne treatment.75,77 randomized controlled trials covering diverse approaches such as Aloe vera,
pyridoxine, fruit-derived acids, kampo (Japanese herbal medicine), and
3. Oral isotretinoin should be first-line therapy for very severe (cystic and
ayurvedic herbal treatments.78 Although mechanisms of potential benefit for
conglobate) acne.75
some were biologically plausible, the included studies were of poor quality and
4. Oral isotretinoin therapy should proceed until full clearance of acne. inconclusive.
Additional studies are needed to define a total cumulative dose that Another systematic review of 17 traditional Chinese medicine randomized
maintains remission. controlled trials found some benefit for acupuncture with moxibustion that was
5. Acne flare with oral isotretinoin can be minimized by initiating therapy at a better than Western medicines, but the quality of included studies was
low dose. limited.78,79
6. Most patients with acne should receive maintenance therapy with a topical A review of studies published from 2007 to 2010 showed most studies were
retinoid. level of evidence grade D. Two studies of grade A concluded that topical tea tree
7. Azelaic acid cream 20% or gel 15% is a useful acne treatment in pregnant oil 5% gel and gluconolactone are efficacious in mild-to-moderate acne, with the
women and patients with acne and PIH. latter agent comparable with benzoyl peroxide 5%. No data supported these
8. At present, devices that use laser, intense pulsed light, or photodynamic claims, and one study predated the review dimensions (published in 1992). Tea
therapy should not be considered first-line treatment for inflammatory acne. tree oil contains terpinen-4-ol, which appears to have some antimicrobial
9. A minority of women 25 years of age have acne lesions localized only to activity. One grade B study compared tea tree oil 5% against benzoyl peroxide
the lower face. Topical retinoids with or without benzoyl peroxide are 5% without placebo and concluded tea tree oil provided slower relief but less
important components in therapy of adult acne. discomfort.80
10. Early and effective treatment is important to minimize potential risk for acne A systematic review of four randomized controlled trials of tea tree oil in
scarring. 2000 did not find conclusive evidence of benefit.81 Tea tree oil continues to be
studied for its efficacy and safety in acne.82,83
General Information Regarding Efficacy and Safety There is increasing interest in the use of CAM as adjuvant or single therapies:
The guidelines and recommendations of the American Academy of Dermatology in America, 7% people report using a complementary medicine, and 2% report
considered the efficacy and safety of various treatments, such as topical agents, seeing a complementary medicine practitioner.84 Traditional Chinese medicine
systemic antibacterial agents, hormonal agents, isotretinoin, miscellaneous has been widely used to treat acne for many years, based on a diagnosis from a
therapies, complementary and alternative therapies, and dietary restriction, based traditional Chinese medicine perspective according to the different syndromes of
on levels of evidence and best clinical practice.74 More specific information acne.
about the efficacy and safety of each of these specific modalities is outlined The Cochrane collaboration undertook a systematic review, reported in 2015,
below in sections on each individual agent. to assess the effectiveness and safety of any CAM in the management of acne
vulgaris.83 This included 35 studies, with a total of 3,227 participants in parallel-
Alternative Drug Treatments group randomized controlled trials (or the first phase data of randomized cross-
over trials) of any kind of CAM, compared with no treatment, placebo, or other
active therapies, in people with a diagnosis of acne vulgaris. The primary demonstrating that glycolic acid is effective and well tolerated in mild-to-
outcome was improvement of clinical signs assessed through skin lesion counts. moderate acne vulgaris.
Some evidence from single studies showed low-glycemic load diet, tea tree oil, Both glycolic acid-based, salicylic acid or salicylic acid derivative-based, (eg,
and pollen bee venom (PBV) may have an effect reducing total skin lesion lipohydroxyacid) and amino fruit acid-peeling preparations have been used in
counts and acne severity scores. However, small sample sizes and poor the treatment of acne. There is very little evidence from clinical trials published
methodological quality limited the strength of the evidence. Evidence from other in peer-reviewed literature supporting the efficacy of peeling regimens.68 Topical
existing randomized controlled trials does not support the use of herbal corneolytics, including retinaldehyde/glycolic acid or lactic acid, induce a
medicine, acupuncture, or wet-cupping therapy for the treatment of acne comedolytic effect and may also facilitate skin absorption of topical drugs.64
vulgaris. The evidence for a secondary outcome (number of participants with Further research on the use of peeling in the treatment of acne needs to be
remission) for herbal medicine versus antibiotic was uncertain. Two trials conducted to establish best practices for this modality.
reported QOL showed the benefit of herbal medicine compared with western
drugs. From the review of 31 studies, the Cochrane review cautioned there is a Hydroquinone To control pigmentation, hydroquinone, which reversibly
lack of evidence to support the use of other CAMs, such as aloe vera, copaiba damages melanocytes, has been used as a hypopigmenting agent in
essential oil, dried fruit of Berberis vulgaris, or seaweed oligosaccharides for the concentrations of 2% to 4%, in preparations of clear or tinted gels, which are
treatment of this condition. Most studies were done in a traditional Chinese more drying, and as vanishing or opaque, flesh-tinted creams, with or without α-
medicine context; therefore, results might be less generalizable to western hydroxy acids or sunscreens. Hydroquinone causes fading of epidermal but not
medicine. The review highlights potential adverse effects from herbal medicine dermal pigmentation. Onset of response is usually 3 to 4 weeks, and the
(dizziness, dry mouth, nausea, diarrhea, or stomach upset); acupuncture (pain, depigmentation lasts for 2 to 6 months but is reversible. While effective in the
itchiness, or redness) and tea tree oil gel (pruritus, dryness, burning sensations, removal of melanin, hydroquinone has been clinically found to be a possible
and skin flaking).83 carcinogen and causes a blue-black discoloration known as ochronosis.87
A 2018 review focused on the use of essential oils and aromatherapy in acne, After considering new data and information on the safety of hydroquinone,
examining existing evidence from small pilot studies.85 It reaffirmed there is the FDA issued a proposed ruling in 2006 about hydroquinone products. The
only weak clinical evidence that tea tree oil 5% may be used as an alternative FDA proposed reversing earlier rules that hydroquinone is generally recognized
acne therapy. Several agents may be helpful as complementary therapy due to as safe and effective. The FDA has not yet issued a final ruling on the status of
biologic plausibility, including lactobacillus-fermented Chamaecyparis obtuse, nonprescription hydroquinone, and many physicians consider a ban unnecessary,
copaiba, sandalwood oil, rosemary extract, jeju essential oil, and Korean citrus, given the lack of convincing evidence of carcinogenic risk to humans and the
but concluded there is little supportive clinical evidence. rarity of ochronosis occurrence.
The use of botanical preparations that are nonstandardized should be Treatment of Scarring Drug and nondrug measures for scar resolution are
discouraged in favor of traditional quality-controlled preparations that have important in acne vulgaris because many patients are scarred despite adequate
evidence of efficacy. The lack of appropriate data, absence of quality treatment and scarring carries an emotional toll. Interventions for atrophic scars
assessment, and inconsistencies in search methodology suggest that CAM cannot might be aided through early identification of patients at risk using a risk
be recommended for acne therapy at this time. assessment tool for scar development. One such tool incorporates four factors:
Glycolic Acid Another agent considered alternative therapy for acne vulgaris is worst ever severity of acne, duration of acne, family history of atrophic acne
glycolic acid. The efficacy and tolerability of a 0.1% retinaldehyde/6% glycolic scars, and lesion manipulation behaviors.88
acid combination (Diacneal) has been evaluated for mild-to-moderate acne Effective procedures for treatment of scarring focus on resurfacing
vulgaris.86 Physician and patient ratings of acne symptom severity and tolerance techniques. For patients with mild scarring, nonprescription α-hydroxy acids
performed at baseline and months 1, 2, and 3 showed mean numbers of papules, may be used, while severe scarring may be corrected with other treatment
pustules, and comedones were significantly reduced from month 1 on, modalities that require consultation with a dermatologist. Dermabrasion, local or
subcuticular excision, collagen implants, chemical peels (eg, 70% glycolic acid, retinoid is added. Azelaic acid 15% gel has also shown good results in a small
trichloroacetic acid), and laser therapy have been used to improve scarring. study. Hormonal therapy, including oral contraceptives (OCs), can play an
Atrophic scars can be treated with laser resurfacing. Usually the scar is not important role in management of acne in women and is typically used in
completely removed, but a more cosmetically acceptable result is achieved. combination with topical acne therapy.73
Keloids and hypertrophic scars can be treated with intralesional triamcinolone, Selecting appropriate treatment in pregnant women can be challenging
cryotherapy, topical steroids, and silicone sheeting. Surgical options for scars because many acne therapies are teratogenic; all topical and especially oral
include excision, augmentation with collagen or fat, chemical peels, subcision, retinoids should be avoided. Oral therapies, such as tetracyclines and
and injection of autologous fibroblasts. antiandrogens, are also contraindicated in pregnancy. Topical and oral treatment
with erythromycin may be considered.
Special Populations Acne in skin of color is an increasing problem, presenting unique challenges.
About 20% of young infants (2-3 months of age) develop papules, pustules, and Postinflammatory hyperpigmentation (PIH), a hypermelanotic reaction to skin
less commonly closed or open comedones, primarily on the cheeks, due to inflammation, is a common occurrence in patients with acne, particularly in
placental transfer of maternal androgens (neonatal acne). The acne subsides those with darker skin and those who excoriate their lesions, affecting all
within a few months with regular maturation. Boys are affected more often than genders and ages. It has a prolonged duration and can be more bothersome than
girls because of a transient increase in testosterone secretion during the third and active acne lesions. Prevention (including sun protection) and early treatment of
fourth month of intrauterine life. Malassezia spp. may be involved in underlying acne-associated inflammation effectively is a primary approach to
pathogenesis.36 Resolution occurs without therapy.89 Infants with neonatal acne PIH management. Chemical peels, lasers, and other light therapies may also be
may have more severe teenage acne.36 used for PIH; however, these methods can also cause pigmentation problems so
should be used with care. Topical retinoids also improve pigmentation by
The treatment of acne in children is similar to treatment for adults. Because
topical therapies may be more irritating in children, initiation with low inhibiting melanosome transfer to keratinocytes and increasing epidermal
concentrations is preferred. Systemic treatments should be reserved for more turnover, lessening pigmentation. It is important for the patient to be aware that
extensive cases. Erythromycin is preferred over tetracyclines for children many PIH lesions resolve spontaneously, but slowly.73
younger than 9 years of age because tetracyclines can affect growing cartilage Although combination therapy is now the standard of care in acne, concerns
and teeth. exist with the increased potential irritation and dryness in skin of color. Although
Although treatment with isotretinoin has numerous potential minor adverse individual medications can be titrated or applied at different times of day to
effects in patients of all ages, an uncommon complication in young patients is avoid irritation, this is not always practical or desirable. There is a paucity of
premature epiphyseal closure. This generally occurs when isotretinoin is clinical studies that evaluate the safety and efficacy of acne medications in skin
administered in high doses, thus limiting long-term therapy. of color. One study has examined susceptibility to irritation in Fitzpatrick skin
types I to III versus types IV to VI and found subjects with darker skin were not
There is a growing population of women seeking acne therapy and a clinical
perception that acne in women requires systemic treatment. Recent analyses of more susceptible and tolerability was comparable across the two groups.
clinical trials have shown that topical therapy can be efficacious in this group. Hispanic subjects were not more susceptible to irritation compared with total
Most patients have an acne presentation similar to adolescent acne, with mixed study groups.90
inflammatory and noninflammatory lesions on multiple facial areas (not limited
to the mandibular area). Topical therapy with a retinoid and antimicrobial can be Drug Class Information
a good option. Data support the use of retinoids, including adapalene/benzoyl This section reviews the pharmacology and mechanisms as related to
peroxide in both 0.1% and 0.3% concentrations, tretinoin 0.04%, and a pathophysiology for pharmacologic options recommended in the guidelines for
retinaldehyde 0.1%/glycolic acid/6% cream. Among antimicrobial agents, both mild, moderate, and severe acne. It will also review evidence of efficacy and
dapsone and clindamycin/benzoyl peroxide have shown efficacy if a topical safety as well as kinetics, interactions, dosing, and administration when relevant.
Topical Therapies Topical therapy agents that are available over the counter or
by prescription. The choice of therapy can be influenced by age of the patient,
site of involvement, extent and severity of disease, and patient preference.
Topical therapies may be used as monotherapy, in combination with other topical
agents, or in combination with oral agents in both initial control and
maintenance. Strength of recommendations for treatment of acne with topical
therapies is shown in Table 113-2. Commonly used topical acne therapies
include benzoyl peroxide, salicylic acid, antibiotics, combination antibiotics with
benzoyl peroxide, retinoids, retinoid with benzoyl peroxide, retinoid with
antibiotic, azelaic acid, and sulfone agents.73
TABLE 113-2 Monitoring of Medications Used in Acne Treatment and
Maintenance Therapy
Salicylic Acid Salicylic acid, a β-hydroxy acid, is a comedolytic agent that is
Exfoliants (Peeling Agents) Exfoliants induce continuous mild drying and available over the counter in 0.5% to 2% strengths. Clinical trials demonstrating
peeling by primary irritation, damaging the superficial layers of the skin, and the efficacy or safety of salicylic acid in acne are limited, although it has been
inciting inflammation. This stimulates mitosis, thickening the epidermis, and used for many years.73 It is a natural ingredient in many plants such as willow
increasing horny cells, scaling, and erythema. A decrease in sweating results in a tree or willow bark, and it penetrates the pilosebaceous unit. The comedolytic
dry, less oily surface and may superficially resolve pustular lesions. action depends on concentration: concentrations in commercial preparations
In the past, a rabbit model was used to study the efficacy of topical exfoliants (<2%-3%) are generally low. Concentrations less than 2% may in fact increase
in retarding tar-induced comedone formation and accelerating their loss keratinization, while those between 3% and 6% are keratolytic, softening the
(comedolysis). In this animal model, retinoic acid (tretinoin) was most active, horny layer and producing shedding of scales. Its mechanism remains
compared with benzoyl peroxide and salicylic acid, which were respectively less unresolved, attributed to either reduced cohesion of corneocytes or shedding of
active. Data from peer-reviewed literature regarding the efficacy of sulfur, epidermal cells, rather than breakdown of keratin.
resorcinol, sodium sulfacetamide, aluminum chloride, and zinc are limited. Salicylic acid has no effect on the mitotic activity of normal epidermis and
Traditional nonprescription exfoliants, including phenol, resorcinol, beta- does not influence disordered cornification.94 It may provide mild antibacterial
naphthol, sulfur, Vleminckx solution, and sodium thiosulfate, are weak or value, as it is active against P. acnes. It offers slight anti-inflammatory activity at
ineffective. These agents are not comedolytic given that they affect the concentrations ranging from 0.5% to 5%. Its efficacy against comedones helps to
superficial epidermis rather than the hair canal. They have been supplanted by prevent development of inflamed lesions, thus providing a delayed efficacy.95
superior effective agents. Linoleic acid-rich phosphatidylcholine combined with
Salicylic acid is effective. As a peeling agent, its relative strength compared
4% nicotinamide is suggested as an emulsion treatment that may be effective in
with others in this class varies according to the model used in measurement. It is
normalization of follicular hyperkeratinization, and also provide anti-
slightly less potent than equal-strength benzoyl peroxide when measured with
inflammatory effects.91,92 the rabbit ear animal model, and slightly more potent when measured with a
Resorcinol Although sulfur and resorcinol have been used for many years in the biologic microcomedone model.95 Its anti-inflammatory properties may help dry
treatment of acne, evidence from peer-reviewed literature supporting their inflammatory lesions.93 Its comedolytic properties are considered less potent
efficacy is lacking.73 The phenol derivative resorcinol is less keratolytic than than topical retinoids. It is often used when patients cannot tolerate a topical
salicylic acid. It is noted to be both bactericidal and fungicidal. Products retinoid because of skin irritation.96
containing resorcinol 1% to 2% have been used for acne, often in combination Its keratolytic effect may enhance the absorption of other agents. Salicylic
with other peeling agents such as sulfur or salicylic acid. The FDA considers acid is a mild irritant and may cause some degree of local skin peeling and
resorcinol 2% and resorcinol monoacetate 3%, in combination with sulfur 3% to discomfort (burning or reddening). It is not a sensitizer. Although the FDA
8%, to be safe and effective and that the combination may enhance the activity recognizes salicylic acid as safe and effective, the compound offers no
of sulfur. However, the FDA is not convinced that resorcinol and resorcinol advantages over more modern topical agents such as benzoyl peroxide.92,94,96
acetate are safe and effective when used as single ingredients, and has placed Salicylic acid products are often used as first-line therapy for mild acne
such products in category II (not generally recognized as safe and effective, or because of their widespread availability without a prescription. They are often
misbranded).92 available in alcohol–detergent impregnated pads as well as washes, bars, and
Resorcinol is an irritant and sensitizer and should not be applied to large areas semisolid vehicles. Both wash-off and leave-on preparations are well tolerated.
of the skin or on broken skin. It produces a reversible, dark brown scale on some Lower concentrations are sometimes combined with sulfur to produce an
dark-skinned individuals. additive keratolytic effect. Concentrations up to 5% to 10% can be used for acne,
Protective packaging is important as resorcinol is reactive to light and beginning with a low concentration and increasing as tolerance to the irritation
oxygen. It has good solubility in both water and alcohol and is heat stabile. Thus, develops. However, the maximum strength allowed in nonprescription acne
it is incorporated into a variety of products, including emulsions.93 products is 2%. In high concentrations of 20% to 30% in hydroethanolic
vehicles, salicylic acid, either alone or in combination, can be used as a peeling topical therapy because of their ability to target key stages in the development of
agent for comedonal acne and hyperpigmentation. It has been shown to extrude the disease: they are comedolytic, resolve the precursor microcomedone lesion,
closed and open comedones several days after peel, but it must be applied under and are anti-inflammatory.
strict control to offer this adjunctive benefit when treating acne vulgaris.97 These agents act to reduce obstruction within the follicle and therefore are
useful in the management of both comedonal and inflammatory acne. As a
Sulfur Sulfur medications often lessen the severity of acne, presumably because group, the retinoids are highly active peelers as they reverse abnormal
of keratolytic and antibacterial action. Sulfur helps to resolve comedones by an
keratinocyte desquamation.99 They improve acne vulgaris by inhibiting
exfoliant action. Its popularity is due to its ability to quickly resolve pustules and
microcomedone formation, diminishing the number of mature comedones and
papules, mask and conceal lesions (as a thick foundation lotion), and produce
subsequently, inflammatory lesions. They also normalize follicular epithelium
irritation leading to skin peeling and mild antibacterial action. Sulfur is used in
maturation and desquamation. The third-generation retinoids (ie, adapalene and
the precipitated or colloidal form in concentrations of 2% to 10%, because it is
tazarotene) are receptor specific. Topical retinoids, unlike isotretinoin, do not
practically insoluble in water and must be well dispersed. Its stability depends on
decrease production of sebum, but primarily decrease inflammation, normalize
effective maintenance of the dispersion.93 Sulfur compounds (eg, sulfides, keratinocyte differentiation, and increase keratinocyte proliferation and
thioglycolates, sulfites, thiols, cysteines, and thioacetates) are also available and
migration.99
somewhat weaker. Sulfur can cause slight ophthalmic and dermatologic
irritation, and patients should be cautioned to avoid eye contact. Use should be Retinoids facilitate acne clearance through secondary effects of loosening and
discontinued if excessive irritation results. Although it is often combined with decreasing corneocytes. This increases skin permeability, facilitates absorption
salicylic acid or resorcinol to increase its effect, its use is limited by its offensive of other agents, such as antimicrobials or benzoyl peroxide, and increases
penetration of oral antibiotics into the follicular canal. As a result, the overall
odor and the availability of more effective agents.98
duration of antibiotic treatment decreases, and the possibility of resistance
Sulfur has met the criteria of the FDA Advisory Review Panel for lessens. Therefore, combination products with oral or topical antimicrobials are
nonprescription topical acne products and is considered safe and effective when available for increased efficacy, faster onset of effects, decreased total antibiotic
used alone, although its antibacterial effects were not recognized by this panel.
use and risk of resistance, and shorter duration of treatment.99 Retinoids may
Sodium thiosulfate, zinc sulfate, and zinc sulfide were not considered safe and
also improve and prevent postinflammatory hyperpigmentation often seen in
effective.
people with darker complexions who have acne.
Topical Retinoids Topical retinoids are prescription vitamin A derivatives with Retinoic acid (vitamin A acid or tretinoin) is a powerful exfoliant that slows
well-documented, randomized, double-blind, placebo-controlled trials the desquamation process, reducing numbers of both microcomedones and
supporting their use for acne treatment.74 Three active agents are available: comedones.31 It is not to be used in pregnant women because of risk to the fetus.
tretinoin (0.025%-0.1% in cream, gel, or microsphere gel vehicles), adapalene Gels and creams are less irritating than solutions.
(0.1%, 0.3% cream, or 0.1% lotion98,99), and tazarotene (0.05%, 0.1% cream, Adapalene is a stable, fast-acting, antiacne treatment that has significant anti-
gel, or foam). Each retinoid binds to a different set of retinoic acid receptors inflammatory and comedolytic properties.99–103 It causes epidermal and
conferring slight differences in activity, tolerability, and efficacy: tretinoin to follicular epithelium hyperplasia, increased desquamation, keratinocyte
alpha, beta, and gamma; and tazarotene and adapalene, selectively, to beta and differentiation, and loosening of corneocyte connections. Its anti-inflammatory
gamma. Binding to specific nuclear receptors reduces inflammation, and inhibits effect is due to the inhibition of oxidative metabolism of arachidonic acid and
sebocyte proliferation and differentiation, which reduces sebum production. inhibition of chemotactic reponses.103 It is better at reducing inflammatory
Retinoids are the most powerful available peeling agents since normal lesions and total lesion count104 and causes less local irritation because of its
epithelial cell differentiation is a vitamin A–dependent process. There is no mechanisms and receptor specificity than tretinoin or tazarotene.101–108 Release
consensus about the relative efficacy of currently available topical retinoids from lotions and hydroalcoholic gels is more effective than from creams and
(tretinoin, adapalene, tazarotene) and oral isotretinoin. Retinoids are the core of aqueous gels and a microsphere gel formulation may be less irritating.99,104 It is
a good first-line therapy for colder climates or in patients with sensitive skin.87 postinflammatory hyperpigmentation due to retinoid dermatitis. To decrease
Adapalene is generally regarded as the topical retinoid of first choice for both irritation, start with the lowest concentration and increase as tolerated.
treatment and maintenance therapy, as it is as effective but less irritating than Application of retinoids should be at night, a half hour after cleansing, starting
other topical retinoids.60,76 It is available in fixed-dose combinations in with every other night for 1 to 2 weeks to adjust to irritation. Short contact time
specialized gel vehicles with benzoyl peroxide to increase the efficacy in starting with 2 minutes and adding 30 seconds per dose can be advised for
comparison with monotherapies. This strategy allows for the synergy of patients with sensitive skin or in the winter, discontinuing and resuming after a
adapalene effects on normalizing desquamation with reduction of inflammation 3-day rest if undue irritation results. Doses can be increased only after beginning
due to benzoyl peroxide action against P. acnes. Adapalene gel 0.1% has been with 4 to 6 weeks of the lowest concentration and least irritating vehicle. Gels
approved as a nonprescription product for once-daily application by patients and creams are less irritating than solutions. Adapalene and tazarotene are photo-
aged 12 years and older. irritants (not photosensitizers), and sun avoidance and sunscreen use are
Tazarotene is also a specific agent with superior efficacy to parent retinoids, imperative.99
reducing both noninflammatory and ILs.53 While its exact mechanism is These agents enhance any other topical acne regimen and allow for
unknown, it is thought to activate retinoid receptors and thereby affect maintenance of clearance after discontinuation of oral therapy. Since retinoids
keratinocyte differentiation, and inhibit proinflammatory transcription factors to are ideal for comedonal acne, when used in combination with other agents, they
decrease cell proliferation and inflammation.53 It penetrates skin but can address all acne variants. Three topical agents are available that contain
accumulates in the upper dermis. It is as effective as adapalene in reducing retinoids in combination with other products: adapalene 0.1%/ benzoyl peroxide
noninflammatory and IL counts when applied half as frequently. Compared with 2.5%, approved for use in patients aged 9 years or older, and two agents with
tretinoin, it is as effective for comedonal and more effective for inflammatory fixed combination clindamycin phosphate 1.2%/tretinoin 0.025% gel, approved
lesions when applied once daily.107–109 Tazarotene foam 0.1% has been studied for those age 12 years or older.73
as an alternative vehicle to the gel with less systemic absorption and is a safe and Some formulations of tretinoin are not photostable and should be applied in
effective formulation.110,111 Tazarotene is not degraded by sunlight.31 the evening. Tretinoin also may be oxidized and inactivated by the
The retinoid class includes the systemic agent isotretinoin, which has effects coadministration of benzoyl peroxide. It is recommended that the two agents be
on comedogenesis and sebum control, and is reviewed below under Antisebum applied at different times. Tretinoin microsphere formulation, adapalene, and
Agents. tazarotene do not have similar restrictions. Topical retinoids have been
associated with an increased risk of photosensitivity; concurrent daily sunscreen
Retinoids tend to produce remissions that are maintained for extended periods
can be used to reduce the risk of sunburn.
of time, provided the accompanying irritation does not impede patient
adherence. Side effects, including dryness, peeling, erythema, and irritation, can The therapy of acne in children younger than 12 years of age with products
be mitigated by reduced frequency of application. Given any single agent, higher approved by the FDA has expanded. Fixed combination benzoyl peroxide
2.5%/adapalene 1% gel is approved for patients 9 years of age or older, and
concentrations may be more efficacious, but with greater side effects. The
tretinoin 0.05% micronized tretinoin gel for patients 10 years of age or older. All
vehicle of any particular retinoid may also decrease tolerability.102,103 Most
other retinoids are approved by the FDA for patients 12 years of age or older.
retinoids are unstable and insoluble in water.
Current data show that retinoids in younger patients are effective and are not
Topical retinoids are not teratogenic; however, tretinoin should be used
associated with increased irritation or risk.73
cautiously in pregnancy and tazarotene is contraindicated. Tretinoin and
adapalene are in FDA category C, while tazarotene, based on large-surface-area Overall, topical retinoids are the cornerstone of acne treatment and provide
safe, effective, and economical means of treating all but the most severe cases of
use in psoriasis (see Chapter 114, “Psoriasis,” is in FDA category X.36
acne vulgaris. They should be the first step in moderate acne, alone or in
Skin type and age may influence tolerability in addition to the choice of combination with antibiotics and benzoyl peroxide, reverting to retinoids alone
vehicle. Oily skin may be more resistant, and darker skin is more prone to for maintenance once adequate results are achieved. Their lack of effect in
inducing bacterial resistance enables long-term maintenance of remission. 5% lowers free fatty acids 50% to 60% after daily application for 14 days and
A Cochrane systematic evidence-based assessment of all issues regarding decreases aerobic bacteria by 84% and anaerobic bacteria (primarily P. acnes) by
acne treatment with topical retinoids is planned to establish optimal treatment 98%.
regimens, compare efficacy and tolerability of combination therapy, assess effect It also produces comedolysis. While earlier rabbit model studies showed a
on P. acnes resistance, and evaluate safety.109 benzoyl peroxide effect greater than that of salicylic acid, these animal
comedones were not physiologic but induced by tar. More recent studies using
Antibacterial Agents Choices for antibacterial therapy include benzoyl native microcomedones show an anticomedogenic effect that is only
peroxide, prescription topical and systemic antibiotics, and combination comparatively slight, compared with tretinoin or salicylic acid.114–116
products. These drugs kill P. acnes and inhibit the production of
Finally, a supplementary benefit of benzoyl peroxide is an indirect anti-
proinflammatory mediators by organisms that are not killed.31 inflammatory action, which is due either to its antibacterial or oxidizing effects.
Benzoyl Peroxide Benzoyl peroxide is a bactericidal agent that has proven This has been reported in several studies and thus can be used to support
effective in the treatment of acne. It kills P. acnes through the release of free treatment of predominantly inflamed lesions.113 The drug’s antiacne effect is
oxygen radicals and is also mildly comedolytic. No resistance to this agent has augmented by increased blood flow, dermal irritation, local anesthetic properties,
been reported, and the addition of benzoyl peroxide to regimens of antibiotic and promotion of healing.117–120 Because the primary effect of benzoyl peroxide
therapy enhances results and may reduce resistance development. is antibacterial, it is most effective for inflammatory acne. Many patients with
Benzoyl peroxide is a derivative of coal tar and was first used for acne noninflammatory comedonal acne will respond to its peeling action.
vulgaris in the mid-1960s, becoming popular once stable formulations aimed at Benzoyl peroxide is available in a variety of preparations such as topical
its heat-lability were developed in the mid-1970s.105 These preparations are the washes, foams, creams, or gels, and can be used as leave-on or wash-off agents.
single most useful group of topical nonprescription drugs. Used alone or in There is no clear superiority of different preparations in terms of effectiveness.
combination, benzoyl peroxide is the standard of care for mild-to-moderate Newer delivery systems to enhance efficacy and tolerability are also being
papular-pustular acne.29,39,73 It is an agent of first choice when combined with investigated. Strengths available for acne therapy range from 2.5% to 10%. Total
adapalene for most patients with mild-to-moderate inflammatory acne vulgaris skin contact time and formulation can affect efficacy. Lower concentrations (eg,
and a second choice alternative for patients with noninflammatory comedonal 2.5%-5%), water-based, and wash-off agents may be better tolerated in patients
acne.29,39,73 A systematic review of 22 trials using benzoyl peroxide for acne with more sensitive skin.
vulgaris provided evidence that it reduces acne-lesion count, although high- Cleansers containing benzoyl peroxide are available as nonprescription liquid
quality evidence is not robust enough for firm conclusions.112 washes and solid bars of various strengths. The desquamative and antibacterial
Benzoyl peroxide is well absorbed through the stratum corneum and effectiveness in a soap or wash is minimized by limited contact time and
removal with proper rinsing. Alcohol and acetone gels facilitate bioavailability
concentrates in the pilosebaceous unit.113 It has three principle actions useful in
and may be more effective, while water-based vehicles are less irritating and
both noninflammatory and inflammatory acne. It produces powerful anaerobic
better tolerated. Paste vehicles are stiffer and more drying than ointments or
antibacterial activity due to slow release of oxygen, thereby acting against gram-
creams, which facilitate absorption and allow the active ingredients to stay
positive and gram-negative bacteria, yeasts, and fungi. This nonspecific
localized.
antibacterial mechanism does not induce resistance with long-term use.113 It has
Concentrations of 2.5%, 5%, and 10% in a water-based gel have been
a rapid (within 2 hours) bactericidal effect that lasts at least 48 hours. As a result,
compared with the vehicle alone. The 2.5% formulation is equivalent to the 5%
it may decrease the number of inflamed lesions within 5 days. As an indirect
and 10% formulation in reducing the number of inflammatory lesions. The lower
effect, it induces suppression of sebum production; it does not reduce skin
strength may not be as effective a peeler compared to higher strengths, which is
surface lipids, but is effective in reducing free fatty acids, which are
due to an irritancy reaction. Thus, irritant side effects with the 2.5% gel are less
comedogenic agents and triggers of inflammation.113 Topical benzoyl peroxide frequent than with the 10% gel but are equivalent to the 5% gel. The lowest
concentration of benzoyl peroxide should be used for treating patients with tolerability advantages over using either agent alone; most trials have assessed
easily irritated skin and may lessen irritation when used in combination topical benzoyl peroxide in combination with clindamycin. Combination with
therapy with comedolytic agents. erythromycin show advantages over oral tetracycline monotherapy.130
Therapy is limited by staining and bleaching of hair, bedsheets, and clothing, The adjunctive use of clindamycin/benzoyl peroxide gel with tazarotene
concentration-dependent irritation, and uncommonly contact allergy. It produces cream promotes greater efficacy and may also enhance tolerability. Increased
a mild primary irritant dermatitis that subsides with continued use and is more tolerability might be attributed to emollients in the clindamycin/benzoyl
likely to occur in those with fair complexions, a tendency to irritancy, or peroxide gel formulation.131 A patented gel formulation of benzoyl peroxide
propensity to sunburn. This irritation is dependent on the concentration and the 5%/clindamycin phosphate 1% (clindamycin) containing dimethicone and
vehicle, being higher with alcoholic gels compared with emulsion bases.114 glycerin was studied both as a monotherapy and in combination with topical
There are rare reports of contact allergic dermatitis. Cross-reactions with other retinoid use. Certain additives, such as silicates and specific humectants, reduced
sensitizers, notably Peruvian balsam and cinnamon, are well established. It may irritation by maintaining barrier integrity.132
cross-sensitize to other benzoic acid derivatives such as topical anesthetics. All single-agent preparations of benzoyl peroxide are now available without
Concomitant use of an abrasive cleanser may initiate or enhance sensitization.121 prescription. Recommend the weakest concentration (2.5%) in a water-based
Another side effect is body odor from breakdown of the benzoyl peroxide that formulation, for anyone with a history of skin irritation, or who must use
remains on clothing and bedsheets. combination therapy.132 There are many suggested routines to initiate therapy.
There is no indication that the normal use of benzoyl peroxide in the One is to gently cleanse the skin and apply the preparation for 15 minutes the
treatment of acne is associated with an increased risk of facial skin cancer. first evening, avoiding the eyes and mucous membranes. A mild stinging and
Although links have been made in experiments with mice, human relevance has reddening will appear. Each evening the time should be doubled until the
not been established. The weak in vitro genotoxic potential is not manifested in product is left on for 4 hours and subsequently all night. Dryness and peeling
vivo based on a lack of initiating or complete carcinogenic activity.113 Overall, will appear after a few days. Once tolerance is achieved, the strength may be
the cutaneous use of benzoyl peroxide is relatively safe, and is recognized by the increased to 5% or the base changed to the acetone or alcohol gels, or to paste.
FDA as category III, which means that more information is required to make a Alternatively, benzoyl peroxide can be applied for 2 hours for four nights, 4
final determination of safety and efficacy for nonprescription use.122–125 Safety hours for four nights, and then left on all night. It is important to wash the
is also confirmed by the American Academy of Dermatology and the German product off in the morning. Other drying agents should be discontinued. Patients
Best Guideline Acne (BGA) Monograph.113 with very sensitive skin or demonstrated sensitivity to benzoyl peroxide should
Benzoyl peroxide has been used in combination with other antiacne not use the product, and it should be discontinued if irritation becomes severe
medications, such as sulfur and chlorhydroxyquinoline, or in formulations with upon use. Contact with eyes, lips, or mouth should be avoided.
urea to facilitate drug delivery. No significant improvement has been A sunscreen is recommended if benzoyl peroxide is used. To avoid
demonstrated. interactions, apply the sunscreen during the day and the benzoyl peroxide at
Benzoyl peroxide has also been combined with prescription agents to night.
improve efficacy, reduce dosing strengths, decrease irritation, and reduce Comparison of Salicylic Acid and Benzoyl Peroxide Although both salicylic
resistance of antibiotics.126–129 acid and benzoyl peroxide are used for mild-to-moderate acne, their mechanisms
Benzoyl peroxide is often combined with topical retinoid for an antimicrobial differ and therefore different types of acne respond to each. Benzoyl peroxide is
effect or used in conjunction with an antimicrobial. It reduces the likelihood of a strong antibacterial agent, while salicylic acid acts primarily through
antibiotic resistance. For long-term maintenance therapy, it is recommended as a keratolysis.
highly efficient bactericidal agent to be added to a topical retinoid.29,39 Studies have shown salicylic acid to be equal or slightly superior to benzoyl
Combining topical antibiotics with benzoyl peroxide has efficacy and peroxide in reducing number of comedones and subsequently number of
inflammatory lesions. Any superiority salicylic acid demonstrates is likely Clindamycin is the preferred macrolide because of potent action, lack of
because it interferes with an earlier step in pathogenesis—formation of the absorption, and its systemic use is limited because it can cause
primary lesion of acne, the microcomedone.94,96 However, studies of the pseudomembranous colitis when given orally or by injection. It is available as a
compound did not use identical formulations. Instead, they compared salicylic single ingredient topical preparation and can also be combined with benzoyl
acid cleansers to benzoyl peroxide washes and salicylic acid solutions to benzoyl peroxide. A topical fixed-dose clindamycin phosphate 12% and benzoyl
peroxide creams. The effect of different bases is critical in determining peroxide 30% combination gel once daily was more effective and twice daily at
differences in efficacy and therefore comparability of action since the base itself least as effective as clindamycin alone twice daily, with an early onset of action
has an effect and influences penetration and duration of action. and an acceptable safety and tolerability profile.135 Erythromycin is available
In summary, the two products have similar efficacy, with salicylic acid noted alone and in combination with retinoic acid or benzoyl peroxide. Stable, fixed-
as stronger in terms of retarding comedone formation. Benzoyl peroxide, as an combination agents are available with erythromycin 3%/benzoyl peroxide 5%,
antibacterial with some peeling effects, is considered the nonprescription and clindamycin 1%/benzoyl peroxide 5%, and clindamycin 1%/benzoyl peroxide
cosmetic gold standard for milder versions of the condition, used alone or in 3.75%. Combination agents may enhance adherence with treatment regimens.
combination to increase efficacy and improve tolerability; however, salicylic Some topical antibiotic–benzoyl peroxide combinations require refrigeration.68
acid is included in many of these products because of the perception of efficacy Tolerance with these agents is excellent; clindamycin alone is pregnancy
and safety for comedonal acne of type 1 or milder presentation.95 category B.74
Other topical antibiotics that are being studied include fluoroquinolones, such
Topical Antibacterials Topical antibiotics for acne accumulate in the follicle,
as 1% nadifloxacin cream, but are not available in the American market.
where they are thought to work through both antibacterial effects (the primary
Research approaches for developing new antibiotics against P. acnes include
mechanism for efficacy in acne) and anti-inflammatory mechanisms. These
combining ribosomal effects of aminoglycosides molecules with bacteria-
agents are best used in combination with benzoyl peroxide (wash-off or leave-
on), which increases efficacy and decreases the development of resistant selective membrane-permeabilizing abilities in one drug.137
bacterial strains. Monotherapy with topical antibiotics in the management of Oral Antibacterials Overview: a systematic evidence-based review of scientific
acne is not recommended because of the development of antibiotic evidence of the efficacy of oral antibiotics for acne was published in 2017. Due
resistance.133,134 Macrolides, including topical erythromycin and topical to heterogeneity in trials, there is insufficient evidence to support one type, dose,
clindamycin, are effective and well-tolerated, well-established acne treatments. or duration of oral antibiotic over another in terms of efficacy and summarized
Clindamycin 1% solution or gel is currently the preferred topical antibiotic key points.138
for acne therapy. Topical erythromycin in 2% concentration is available as a
• The use of oral antibiotics is reserved for patients with moderate-to-severe
cream, gel, lotion, or pledget, but it has reduced efficacy in comparison with
inflammatory acne.
clindamycin because of resistance of cutaneous staphylococci and P. acnes.74
Findings suggest topical erythromycin use for acne has essentially ceased. By • Tetracyclines are considered first-line therapy, while macrolides and
contrast, clindamycin use is increasing.135 More than 50% of Propioni bacterium trimethoprim/sulfamethoxazole are acceptable alternative agents.
acnes strains are resistant to topical macrolides. Resistant strains are usually • It is recommended that oral antibiotics be prescribed with concurrent
resistant to all macrolides.136 topical therapy for improved efficacy and to combat antibiotic resistance.
Current recommendations discourage topical antibiotic monotherapy in favor • The choice of antibiotic should be determined based on the side effect
of combination therapy with benzoyl peroxide and topical retinoids. Addition of profile, resistance, cost, and consensus guidelines.
benzoyl peroxide or topical retinoids to the macrolide antibiotic regimen is more
• Oral antibiotics used in the treatment of acne may have unintended effects
effective than monotherapy and mitigates against survival of resistant P. acnes
populations. on nontarget bacteria, and the clinical implications of this warrant further
exploration.
Systemic antibiotics are a standard of care in the management of moderate The Cochrane collaboration has conducted a review into the efficacy and
and severe acne and treatment-resistant forms of inflammatory acne. There is safety of minocycline, examining 39 randomized controlled trials. These studies
evidence to support the use of tetracycline, doxycycline, minocycline, show that minocycline is an effective treatment for moderate-to-severe
erythromycin, trimethoprim-sulfamethoxazole, trimethoprim, and azithromycin. inflammatory acne but present no evidence to support the first-line use of
Studies do not exist for the use of ampicillin, amoxicillin, or cephalexin. minocycline in acne treatment. The drug is more lipophilic, may act more
However, any antibiotic that can reduce the P. acnes population in vivo and quickly, and can be taken once daily. However, people treated with minocycline
interfere with the organism’s ability to generate inflammatory agents should be are at a significantly greater risk of developing an autoimmune syndrome than
effective.68 Although erythromycin is effective, use should be limited to those those given tetracycline or no treatment.142
who cannot use one of the tetracyclines (ie, pregnant women or children under 8 Sarecycline (Seysara) is a new, oral, narrow-spectrum tetracycline-derived
years of age because of the potential for damage to the skeleton or teeth). antibiotic with anti-inflammatory properties. It is specifically indicated for the
Ciprofloxacin, trimethoprim-sulfamethoxazole, and trimethoprim alone are also treatment of inflammatory lesions of non-nodular moderate-to-severe acne
effective in instances where other antibiotics cannot be used or for patients who vulgaris in patients 9 years of age or older. The mechanism of action of in
do not respond to conventional treatment.92,139 A comparison of azithromycin treating acne vulgaris is not known. Sarecycline should be taken once daily, with
with doxycycline reported doxycycline is a better option for treatment of acne or without food, and the recommended daily dose is based on the patient’s body
vulgaris.140 weight (60 mg if 33-54 kg, 100 mg if 55-84 kg, and 150 mg if 85-136 kg). To
The tetracycline antibiotic family has multiple modes of action, well- reduce the risk of esophageal irritation and ulceration, sarecycline should be
understood antibacterial effects, and anti-inflammatory effects that target an administered with adequate amounts of fluid.
additional aspect of pathogenesis.133,139,141 Agents, such as tetracycline, The FDA approval of sarecycline in October 2018 was based on two
minocycline, and doxycycline, are used only as systemic agents. Through identically designed, large, multicenter, randomized, double-blind, placebo-
calcium chelation, they inhibit neutrophil and monocyte chemotaxis. controlled, phase III studies that assessed use in a total of 2,002 participants 9
Concentrations below the antibiotic threshold still inhibit inflammation and years of age or older with moderate-to-severe facial acne vulgaris. Data
improve both acne vulgaris and acne rosacea. demonstrated that once-daily sarecycline 1.5 mg/kg significantly improved acne
Tetracycline is no longer the drug of choice in this family; its disadvantages severity based on Investigator’s Global Assessment (IGA) success and
include diet-related effects on absorption and the drug’s lower anti-inflammatory significantly reduced inflammatory lesion count versus placebo at week 12.
and antibacterial activity. Study 1: IGA success, 21.9% versus 10.5%, and mean absolute reduction in
The incidence of significant adverse effects with oral antibiotic use is low. number of inflammatory lesions, 15.3 versus 10.2. Study 2: IGA success, 22.6%
However, adverse effect profiles may be helpful for each systemic antibiotic versus 15.3%, and mean absolute reduction in inflammatory lesions, 15.5 versus
used in the treatment of acne. Vaginal candidiasis may complicate the use of all 11.1.143–145
oral antibiotics.68 Doxycycline is very commonly a photosensitizer especially at The majority of oral antibiotic course durations follow guidelines. Costs of
higher doses. antibiotic therapy are reported lower for shorter courses and those using generic
Minocycline has been associated with pigment deposition in the skin, mucous medications.146
membranes, and teeth, particularly among patients receiving long-term therapy Bacterial resistance to antibiotics It is an increasing problem particularly
and/or higher doses of the medication. In some instances this is irreversible. because therapy is directed at control over a long period of time.133 The
Pigmentation occurs most often in acne scars, anterior shins, and mucous development of strains with unidentified mutations suggest new mechanisms of
membranes. Minocycline may cause dose-related dizziness, which resolves with resistance are evolving. Combined resistance to clindamycin and erythromycin is
dose titration; urticaria; hypersensitivity syndrome, autoimmune hepatitis, a much more common than resistance to tetracycline. Use of topical antibiotics
systemic lupus erythematosus-like syndrome; and serum sickness-like can lead to resistance largely confined to the skin of treated sites, whereas oral
reactions.68,133 antibiotics can lead to resistance in commensal flora at all body sites. Resistance
is more common in patients with moderate-to-severe acne and in countries with possible with broad-spectrum antibacterial agents such as benzoyl peroxide. In
high outpatient antibiotic sales. Resistance is disseminated primarily by person- addition, isotretinoin use should be initiated earlier in indicated patients, rather
to-person contact, and thus the spread occurs frequently. than prolonging antibiotic courses.29,75
There have been an increasing number of reports of systemic infections
caused by resistant P. acnes in nonacne patients after surgery. A transmission of Azelaic Acid Azelaic acid is mildly effective as a comedolytic, antibacterial, and
factors conferring resistance to bacteria other than P. acnes has been described. anti-inflammatory agent. The agent has been used in patients with sensitive skin
or of Fitzpatrick skin types IV or greater because of the lightening effect of the
The most likely effect of resistance is to reduce the clinical efficacy of
antibiotic-based treatment regimens to a level below that in patients with fully product on dyspigmentation.73
susceptible flora. This has been shown as a decreased clinical efficacy of topical Azelaic acid possesses activity against all four pathogenic factors that
erythromycin in clinical trials; there is no evidence to date of this effect in produce acne. It has anti-inflammatory and antibacterial activities. Azelaic acid
treatments with oral tetracycline or topical clindamycin. also normalizes keratinization, which accounts for its anticomedogenic effect. It
Studies on P. acnes resistance have highlighted the need for treatment is a competitive inhibitor of mitochondrial oxidoreductases and of 5-α-reductase,
guidelines to restrict the use of antibiotics to limit the emergence of resistant inhibiting the conversion of testosterone to 5-dehydrotestosterone. It also
strains. Patients with less severe forms of acne should not be treated with oral possesses bacteriostatic activity to both aerobic and anaerobic bacteria including
antibiotics, and where possible such therapy should be limited to the shortest P. acnes. Azelaic acid is an antikeratinizing agent, displaying antiproliferative
feasible duration (eg, 6-8 weeks). Local patterns of resistance should be cytostatic effects on keratinocytes and modulating the early and terminal phases
considered.130 The use of systemic antibiotics should be limited (both indication of epidermal differentiation.117 It may produce hypopigmentation. Inhibition of
and duration) and topical antibiotic monotherapy should be avoided. thioredoxin reductase by azelaic acid provides a rationale for its depigmenting
property.
There should be early use of combination therapy with retinoids. Often, when
oral antibiotics are combined with topical agents, the antibiotic may be Azelaic acid 20% cream is used in the treatment of mild-to-moderate
inflammatory acne, has an excellent safety profile with minimal adverse effects,
discontinued after 6 months of therapy.147 Nearly 70% of patients with acne
and is well-tolerated in comparison with other acne treatments. The most
require antibiotics for 12 weeks or less if aggressive retinoid therapy is used
common adverse effects, occurring in approximately 1% to 5% of patients, are
during that time.133 pruritus, burning, stinging, and tingling. Adverse reactions are generally
Another potential strategy that had been suggested is to eliminate the use of transient and mild in nature. Other adverse reactions, such as erythema, dryness,
antibiotics and combine other topical agents. Neither retinoids nor benzoyl rash, peeling, irritation, dermatitis, and contact dermatitis, have been reported in
peroxide creates selective pressure for resistance and is one combination option. less than 1% of patients.150
Although this approach has been evaluated for efficacy and safety, there is
Azelaic acid has been shown effective in clinical trials studied with topical
limited evidence of its effect on microbial resistance. In one open label study of
2% erythromycin, topical 5% benzoyl peroxide gel, and topical 0.05% tretinoin
adapalene and benzoyl peroxide, baseline counts of antibiotic resistant strains of
cream in the treatment of mild-to-moderate inflammatory acne. However, the
P. acnes were reduced by week 4.133
agent has limited efficacy, compared with other antiacne therapies.68 It is an
The high sensitivity of P. acnes to acidified nitrite suggests a useful role in the alternative to first choice therapy for comedonal and all types inflammatory
treatment of antibiotic resistant acne. Nitric oxide and its intermediates diffuse as acne, particularly in combination. It is an alternative to topical retinoids for
well as oxygen and would be expected to penetrate the inflammatory lesions maintenance therapy as its efficacy and safety profile are advantageous for long-
well. The newly developed topical nitric oxide–releasing agent holds potential in
term therapy.29,39,73
limiting antibiotic resistance.148 Further work to optimize the pharmacokinetic
Azelaic acid should be applied twice a day, in the morning and evening. A
delivery of nitric oxide releasers could increase bactericidal effectiveness.149 majority of patients with inflammatory lesions may experience an improvement
Stricter cross-infection control measures are recommended when assessing in their acne within 4 weeks of beginning treatment. However, treatment may be
acne. Any topical or systemic antibiotic therapy should be combined when
continued over several months, if necessary. injection with corticosteroids (eg, triamcinolone acetonide) is a well-established
Azelaic acid is in a pregnancy category B and should only be used in and recognized treatment for large inflammatory lesions. Cystic acne improved
pregnant women if medically necessary. Patients with dark complexions should in patients receiving intralesional steroids.68 Rapid improvement and decreased
be monitored for early signs of hypopigmentation. pain are noted.
Systemic absorption of steroids may occur with intralesional injections.
Dapsone Topical dapsone, a synthetic sulfone, is available as an agent for acne.
Adrenal suppression was observed in one study. The injection of intralesional
Sulfones have both anti-inflammatory and antibacterial properties and may be
steroids may be associated with local atrophy. Lowering the concentration and/or
used in sulfonamide-allergic patients. Dapsone’s utility is attributable to its anti-
volume of steroid may minimize these complications.
inflammatory and antimicrobial properties that improve both inflammatory and
noninflammatory acne, with more prominent effects occurring in inflammatory Antisebum Agents No topical agents directly influence the production of
lesions. In clinical trials, topical dapsone showed modest-to-moderate efficacy, sebum. Systemic drugs that influence sebum production include high-dose
primarily in the reduction of inflammatory lesions.181 Short- and long-term estrogens, antiandrogens (cyproterone acetate), spironolactone, and the retinoid
safety and efficacy have been demonstrated.151,152 isotretinoin. Antioxidants, such as sodium l-ascorbyl-2-phosphate 5%, may act
Topical dapsone gel 5% was shown to be safe, minimally irritating, and to prevent the oxidation of sebum and studies are in preliminary stages.
effective after 12 weeks in the treatment of mild-to-moderate inflammatory Oral antiandrogens, such as spironolactone and cyproterone acetate, can also
facial acne in 101 adult women with sensitive skin.153 The response to dapsone be useful in the treatment of acne. Flutamide is a nonsteroidal selective androgen
5% gel appears to be influenced by gender, with female patients experiencing a receptor blocker used in the treatment of prostate cancer. It is not approved by
significantly greater reduction in acne lesion counts and a significantly higher the FDA for use in acne. While flutamide can be effective, hepatotoxicity is
clinical success rate following 12 weeks of treatment.154 limiting. There is no evidence to support the use of finasteride. Use of flutamide
Topical dapsone 5% gel is available as a twice-daily agent for acne. Dapsone in the treatment of acne is discouraged except where benefit warrants the risk.74
7.5% gel is a once-daily reformulation of the 5% product administered twice There are limited data to support the effectiveness of oral corticosteroids in
daily. It received FDA approval for use in patients aged 12 years and older based the treatment of acne. Oral corticosteroid therapy is of temporary benefit in
on two 12-week, double-blind, placebo-controlled, randomized trials totaling patients who have severe inflammatory acne. In patients who have well-
more than 4,300 patients with acne. The studies showed the stronger once-daily documented adrenal hyperandrogenism, low-dose oral corticosteroids may be
product was extremely well tolerated, with application site dryness and itching useful in treatment of acne.68
rates similar to placebo. In terms of efficacy, a Global Acne Assessment Score of
Oral Contraceptives Estrogen-containing oral contraceptives can be useful in the
0 or 1 with at least a two-grade improvement was achieved in 30% of patients
treatment of acne in some women. Those currently approved by the FDA for the
assigned to dapsone 7.5% gel, compared with 21% of vehicle-treated controls.155 management of acne contain norgestimate with ethinyl estradiol and
Topical dapsone is a novel addition to the treatment armamentarium, norethindrone acetate with ethinyl estradiol. There is good evidence and
especially for patients exhibiting sensitivities or intolerance to conventional consensus opinion that other estrogen-containing oral contraceptives are also
antiacne agents.156 equally effective.68
Combination therapy with dapsone and topical retinoids may be indicated if The mechanism of action of combination oral contraceptives (COCs) in the
comedonal components are present. Topical dapsone 5%, alone or in treatment of acne is based on their antiandrogenic properties. These hormones
combination, with adapalene 0.1% or benzoyl peroxide 4% has been shown to be decrease androgen production at the level of the ovary and also increase sex
safe and efficacious but may be more irritating than other topical agents.157,158 hormone-binding globulin, binding free circulating testosterone and rendering it
Intralesional Steroids Intralesional corticosteroid injections are effective in the unavailable to bind and activate the androgen receptor. In addition, COCs reduce
treatment of individual inflammatory acne nodules. The effect of intralesional 5-alfa-reductase activity and block the androgen receptor.74
The risks of COCs must be weighed against the risks of the condition that
they are treating or preventing. If COCs are used exclusively for acne, their risks Spironolactone At higher doses, spironolactone is an antiandrogenic compound
must be compared to the risks of acne. It is important to remember that FDA that decreases testosterone production and competitively inhibits binding of
approval of all COCs for acne specifies that they are approved for the treatment testosterone and dihydrotestosterone to androgen receptors in the skin. Dosages
of acne in women who also desire contraception. COCs carry cardiovascular of 50 to 200 mg have been shown to be effective in acne. Spironolactone may
risks, and breast cancer risks in some women, and low estrogen may affect bone cause hyperkalemia, particularly when higher doses are prescribed or when there
mass. However, decreased risks of colorectal, ovarian, and endometrial cancers is cardiac or renal compromise. It occasionally causes menstrual irregularity. A
have been shown. 5% spironolactone gel, studied in patients with increased sebum secretion,
Oral contraceptives may improve acne for many women with clinical and resulted in a decrease in the total acne lesions with no significant efficacy under
laboratory findings of hyperandrogenism and in women without these findings. the acne severity index.160 Its use as an antiandrogen is not approved by the FDA
They may be used alone or in combination with other acne treatments.74 for the treatment of acne. Given the small number and size of available studies, a
The Cochrane collaboration conducted a review in 2012 to determine the 2009 Cochrane database review concluded that there are insufficient data to
effectiveness of COCs for the treatment of facial acne compared with placebo or support the efficacy of spironolactone in the treatment of acne. Despite the lack
other active therapies. Thirty-one trials with a total of 12,579 women were of published data, relying on available evidence, experience, and expert opinion,
reviewed.158 the 2016 AAD work group supports the use of spironolactone in the
Combination oral contraceptive use reduced inflammatory and management of acne in select women.74
noninflammatory facial lesion counts, severity grades, and self-assessed acne in Cyproterone Acetate Cyproterone combined with ethinyl estradiol (in the form
nine placebo comparison trials, according to the review. Progestins included of an oral contraceptive) has been found effective in the treatment of acne in
levonorgestrel, norethindrone acetate, norgestimate, drospirenone, dienogest, and females. Higher doses have been found more effective than lower doses. No
chlormadinone acetate. There were fewer clear differences in trials that cyproterone/estrogen-containing oral contraceptives are approved for use in the
compared varying progestin types, showing no superiority, little differences, or United States.158
conflicting results. No conclusions could be reached regarding the effect of a
COC compared with an antibiotic because there was only one underpowered Oral Corticosteroids Oral corticosteroids have two potential modes of activity in
trial.158 the treatment of acne. One study demonstrated that low-dose corticosteroids
Most studies assessed women over six treatment cycles, which might not be suppress adrenal activity in patients who have proven adrenal hyperactivity.161
adequate for a chronic condition like acne. In two trials, patients were more Low-dose prednisone in doses ranging from 5 to 15 mg daily, administered alone
likely to discontinue because of adverse events, suggesting even if COCs or with high estrogen containing COCs, has shown efficacy in the treatment of
improve acne, women might not be willing to accept long-term use for acne acne and seborrhea. Expert opinion is that short courses of higher dose oral
because of other side effects. corticosteroids may be beneficial in patients with highly inflammatory disease.
The review concluded that COCs should be considered for women with acne Long-term adverse effects of corticosteroids prohibit use as a primary therapy
who also want an oral contraceptive. for acne.74
A meta-analysis review of 32 randomized controlled trials comparing use of
Oral Isotretinoin Isotretinoin revolutionized the treatment of acne, yet its use
antibiotics to oral contraceptive agents for acne concluded that although
and availability are increasingly complex. The risk of potential adverse effects
antibiotics may be superior at 3 months, oral contraceptive agents are equivalent
must be weighed against its ability to prevent lifelong and permanent physical
to antibiotics at 6 months in reducing acne lesions and may be a better first-line
and psychologic scarring.162
alternative to systemic antibiotics for long-term acne management in women.159
Oral isotretinoin, an isomer of retinoic acid, has been used in the United
There is a need for more research into comparative effectiveness of COCs in
States for the treatment of acne for more than 30 years and is approved by the
randomized control trials, and into the acceptability and need for long-term use
FDA for the treatment of severe recalcitrant acne vulgaris. Its use has proven
of COCs for acne.158
successful for most patients with severe acne, resulting in decreased sebum In the most severe cases of acne, consideration of pretreatment with oral
production, acne lesions, and acne scarring, along with a decrease in symptoms corticosteroids may also be appropriate. Some patients experience a relapse of
of anxiety and depression. It has also been effectively used in the treatment of acne after the first course of treatment with isotretinoin. Relapses are more
moderate acne that is either treatment-resistant or that relapses quickly after the common in younger adults or when lower doses are used.
discontinuation of oral antibiotic therapy.68 It is the consensus of the 2016 AAD The 2016 AAD guidelines supports initiation of isotretinoin at 0.5 mg/kg/day
guidelines that the presence of moderate acne that is either treatment-resistant or when appropriate, subsequently increasing to a full dose of 1 mg/kg/day after the
that produces physical scarring or significant psychosocial distress is an first month as tolerated, with a goal cumulative dose between 120 and 150
indication for treatment with oral isotretinoin.74 mg/kg. One recent study of 116 patients found that a cumulative dose of 220
A good understanding of this agent’s mechanisms and adverse effects is mg/kg or more may result in lower relapse rates, but confirmation will require
important. Oral isotretinoin is a natural metabolite of vitamin A. Its mechanism study in larger populations.74
is elusive, as it does not bind to retinoid receptors. It has been shown to reduce Isotretinoin is highly lipophilic and is best absorbed when taken with food.
sebogenesis and may also inhibit sebaceous gland activity, growth of P. acnes, One novel formulation is less dependent on the presence of fat in the gut for
inflammation, and improve follicular epithelial differentiation.163 Systemic absorption.167 When used, drying agents must be discontinued and replaced with
isotretinoin exerts a primary effect on comedogenesis, causing a decrease in size moisturizers.
and reduction in formation of new comedones.31 Isotretinoin is the only drug Because isotretinoin is a vitamin A derivative, it interacts with many of the
treatment for acne that produces prolonged remission. biologic systems of the body, and consequently has a significant pattern of
The teratogenic effects of oral retinoid therapy are well documented. Because adverse effects. The pattern is similar to that seen in hypervitaminosis A. Side
of its teratogenicity and the potential for many other adverse effects, this drug effects include those of the mucocutaneous (most common), musculoskeletal,
should be prescribed only by those physicians knowledgeable in its appropriate and ophthalmic systems, as well as headaches and central nervous system
administration and monitoring. Female patients of child-bearing potential must effects. Most of the adverse effects, such as cheilitis and dry nose, eyes, and
only be treated with oral isotretinoin if they are participating in the approved mouth, are temporary and resolve after the drug is discontinued.162 Laboratory
pregnancy prevention and management program (ie, iPLEDGE). Two different monitoring during therapy should include triglycerides, cholesterol,
forms of contraception must be started 1 month before and continue at least 1 transaminases, and complete blood counts.
month (but normally 4 months) after therapy and pregnancy monitoring Mood disorders, depression, suicidal ideation, and suicides have been
undertaken before, during, and after therapy.162 reported sporadically in patients taking this drug. A causal relationship has not
The efficacy of conventional isotretinoin treatment (0.5-1.0 mg/kg/day for 16- been established. These symptoms are quite common in adolescents and young
32 weeks, reaching a cumulative dose of 120 mg/kg) for acne has been well adults, the age range of patients who are likely to receive isotretinoin.
established. The approved dosage of isotretinoin is 0.5 to 2.0 mg/kg/day. The Issues regarding responsible and informed use Published data and expert
drug is usually given over a 20-week course. opinion differ with respect to the use of isotretinoin as first-line or reserve
Initial flaring can be minimized with a beginning isotretinoin dose of 0.5 therapy, optimal dosing, and risk of depression.162
mg/kg/day or less. There are many reports regarding the efficacy of low-dose Although some persist in reserving isotretinoin use only for severe acne,
and intermittent isotretinoin treatment. Lower doses can be used for longer time nodular or conglobate acne that has not responded to appropriate antibiotics and
periods, with a total cumulative dose of 120 to 150 mg/kg or the dose can be topical therapy, delaying use of isotretinoin, the most effective choice, poses an
lowered to 20 mg on alternate days after an initial 2 months of therapy with ethical problem.168 Opinions vary on whether or not to restrict use to patients
higher dosage.164–166 Reports suggest that low-dose regimens are superior to under 12 years and whether to avoid lasers, peelers, or wax epilation for at least
other regimens (conventional or intermittent) in terms of patient satisfaction, 6 months after discontinuation of therapy.169
tolerability, and efficacy for patients with moderate acne. In patients with The causal relationship between the use of isotretinoin and risk of depression
severely inflamed acne, an even greater initial dose reduction may be required. continues to be scrutinized with no consensus. The issue is complex as
depression and suicidal ideation occur with severe acne in the absence of individual patient.74,170,171
isotretinoin.
There are instances in which withdrawal of isotretinoin has resulted in Light Therapy Light therapies are believed to work by killing P. acnes and by
improved mood, and reintroduction of isotretinoin has resulted in the return of damaging and shrinking sebaceous glands, reducing sebum output and have
mood changes. Treatment of severe acne with isotretinoin is often associated few175 or temporary176,177 adverse effects. Light therapies may be used once or
with mood improvement.68 There is epidemiologic evidence that the incidence twice weekly as a course of 6 to 10 treatments, with each irradiation lasting 10 to
of these events is lower in patients treated with isotretinoin than in an age- 20 minutes.177 P. acnes produce endogenous porphyrins that absorb light to form
matched general population. There is also evidence that the risk of depressed highly reactive singlet oxygen, which destroys the bacteria.177 There is still
mood is no greater during isotretinoin therapy than during therapy of an age- debate about the effectiveness of different wavelengths.177 Since porphyrins
matched acne group treated with conservative therapy.68 have peak absorption at blue light wavelengths, blue light is often used to treat
A systematic review published in 2005 did not find any evidence to support acne. Red light is also absorbed by porphyrins and can penetrate deeper into the
worsening of depression after use, and some depressive scores improved with skin,178 where it may directly affect inflammatory mediators. Other light
use; however, nine of these studies had limitations.170 A retrospective cohort therapies attempt to selectively target and damage sebaceous glands directly,
study in Sweden found attempted suicide increased in users, but an increased reducing their size and thus sebum output.179 These include infrared lasers, low-
risk was present before treatment. An increased risk of attempted suicide was energy pulsed dye lasers, and radiofrequency devices.177
present 6 months after isotretinoin, suggesting patients should be monitored for Photodynamic therapy (PDT) uses specific light-activating creams, which are
suicidal behavior after treatment discontinuation.171 A 2016 review on absorbed into the skin and amplify the response to light therapy but tend to
isotretinoin controversies, facts, and recommendations concluded despite produce more severe adverse effects. There are concerns that PDT may interfere
common misperceptions, there is weak evidence for increased incidence of with the skin’s natural immune mechanisms180,181 and cause long-term skin
depression, suicidality, or inflammatory bowel disease with isotretinoin use and damage.
data indicate that transient increases in transaminases and lipid levels do not Light therapies, previously expensive and accessed privately via
typically necessitate discontinuation of therapy.172 dermatologists or clinics, are increasingly popular. Home-use blue light therapy
In 2017, a systematic review and meta-analysis of the literature, with 31 is now available. Patients find it easier to comply with light treatments because
studies, concluded isotretinoin treatment for acne did not appear to be associated of their short duration.
with an increased risk for depression and that the treatment of acne appears to Very few trials compare light therapy with conventional acne treatments. The
ameliorate depressive symptoms.173 Current literature regarding the association European evidence-based guidelines concluded published evidence is scarce and
with depression and suicide was reexamined in 2018. It reconfirmed that while standardized treatment protocols and widespread experience are lacking. Due to
those with a personal or family history of mental disorder might be at risk, conflicting or insufficient evidence, these guidelines did not make a
further studies are needed and no conclusions can be drawn.174 The current recommendation for or against treatment of comedonal, MMPP, or severe
literature is insufficient to support a meaningful causative association, but papulopustular/nodular acne with monotherapy visible light, visible or infrared
important study limitations exist. In the absence of definitive evidence, an wavelength lasers, or intense pulsed light or PDT. Blue light has a low strength
idiosyncratic effect cannot be excluded. This disputed association remains an recommendation as a consideration for MMPP.29,75 An ongoing Cochrane
important area for future research. Given the prevalence of depression, anxiety, review protocol continues to investigate the current state of evidence for use of
and suicidal ideation/suicide in the general population, and especially the light therapy in acne.182
adolescent population who may be candidates for isotretinoin therapy, the
prescribing physician should continue to monitor for these symptoms at each Pharmacologic Cleansing Options
visit for early recognition, advise patients about a possible risk of depression and Medicated Soaps and Washes Medicated soaps, washes, and foams may
suicidal behavior, and make therapeutic decisions within the context of each
contain topical antiseptics such as triclosan; peeling agents such as salicylic acid, validated antikeratinization agents such as retinoids.55
sulfur; antimicrobials such as benzoyl peroxide, clindamycin, or azelaic acid, Alcohol-detergent medicated pads, impregnated with salicylic acid 0.5%,
alone or in combination in low concentrations. They may be nonprescription or have reduced inflammatory lesions and open comedones in mild-to-moderate
prescription status.183 Most washes should remain on the skin from 15 seconds acne. This type of medication is less abrasive, not rinsed off, and convenient.186
to 5 minutes followed by thorough rinsing. This limits the amount of time the Alcohol-detergent wipes, swabs, or “pledgets” impregnated with antibiotics,
active ingredient is in contact with the skin. Other cleansers are applied after such as clindamycin or lincomycin, are available. The antibiotic is deposited in
washing and left on the skin without rinsing. low concentrations on the surface of the skin and may not penetrate to the depths
Quaternary ammonium compounds are cationic detergents that are inactivated of the pilosebaceous duct. Although patients may like the convenience and
quickly in the presence of organic material such as sebum. The duration of perception of using an active agent, they should not be recommended over
action of these products is short. simple cleansing.
Antiseptic cleansers that have been studied include hexachlorophene, Abrasives consist of finely divided particles of fused aluminum or plastic
chlorhexidine, and povidone-iodine. Use of hexachlorophene has since been together with cleansing and wetting agents. Abrasives peel and remove surface
banned in nonprescription products by the UFDA because of neurotoxicity debris and may assist resorption of papules and pustules. Despite vigorous
concerns. Bacteriostatic soaps containing hexachlorophene, carbanilides, and rubbing, removal of comedones is not accomplished. Particles containing active
salicylanilides (halogenated hydroxyphenols) may alter normal flora or be agents, such as sodium tetraborate decahydrate, dissolve on use, and their
acnegenic. Few ordinary soaps induce acne. However, acne patients are abrasiveness is therefore limited.186 The effectiveness of an abrasive cleanser
particularly susceptible to comedogenic contactants, and if these soaps are with and without polyethylene granules showed no difference in results in
applied several times daily for long periods, they may become troublesome. patients with mild-to-moderate acne. These products are not indicated in most
Soaps containing coal tar, which can induce folliculitis, are not indicated for cases but may be used in a patient who responds empirically.187
acne.
In a very small group of patients in an 8-week, double-blind, randomized Personalized Pharmacotherapy
clinical trial, a combination cleanser containing triclosan, azelaic acid, and
salicylic acid produced a greater histopathologic decrease in inflammatory The individualized treatment of certain patient groups, including infants,
response compared with a nonmedicated cleanser, but there was no significant children, pregnant women, and persons of color, is described under Special
Populations.
difference in noninflammatory lesions in either group.184 A rebound tendency
was noted for the nonmedicated cleanser with respect to inflammatory lesions at Providers and patients must also weigh costs and drug availability in choosing
4 weeks. Authors concluded that nonmedicated cleansers were an easier and a treatment regimen. One study showed that the average total cost of treatment
cheaper way of managing patients with mild acne. per episode across all age groups is US $689.06.188 Topical retinoids and fixed-
dose combination therapies are in general more expensive than benzoyl peroxide
Chlorhexidine inhibits in vitro growth of P. acnes.185 A 4% chlorhexidine
preparations. A retrospective analysis investigated adherence to oral antibiotic
gluconate preparation in a detergent base has been shown to be as effective as
guideline recommendations and opportunities for cost-savings. Of 17,448
benzoyl peroxide washes in patients with mild acne, and both preparations
courses, 84.5% aligned with duration guidelines, although 69.0% of courses did
reduced the number of inflammatory and noninflammatory lesions after 8 and 12
not include concomitant topical retinoid therapy. Costs of antibiotic therapy were
weeks, compared with vehicle alone.184 However, further evidence is lacking,
lower for shorter courses and those using generic medications. Mean savings of
and irritation is a side effect.55 $592.26 per person could result if prolonged courses met guidelines.189
Glycolic 1%, an alpha-hydroxy acid (AHA), has been used as a cleanser. Laser treatments and cosmetic procedures are also very costly. The economics
Alpha-hydroxy acids cause desquamation by decreasing basal corneocyte
of long-term maintenance therapy should be borne in mind when selecting a
cohesion and limiting follicular occlusion. AHA-containing formulations may be regimen. Patients should not spend large amounts on herbals and botanicals, as
considered in the treatment of acne in light of mechanistic similarities with better
well as home remedies, given the lack of current good evidence to support their benefit to QOL. Clinicians should review patient understanding of each of these
use. As acne is a chronic disease extending over many years, total cost important factors to ensure patient adherence. There is often a need to
implications are important and affect adherence and response. supplement counseling sessions with written materials to which the patient can
Other practical considerations include the need for refrigeration of some refer at home.
products such as antibiotics. Local patterns of resistance should be kept in mind Good adherence is the key to treatment success. Other strategies to increase
in choosing antibiotics. Extent and area of lesion involvement when large or adherence include use of once-daily regimens, online follow-up visits, and
inaccessible (eg, the back or trunk) as well as ease of application may determine remote digital imaging for ongoing lesion assessment.188,191,192 A randomized
the choice of route between topical and systemic therapy. The natural skin controlled trial compared the effectiveness of automated online counseling to
predilection toward oiliness versus dryness may dictate the choice of vehicle. standard web-based education on improving acne knowledge. While both
Dietary interactions should be born in mind with certain drugs such as oral models had a significant increase in knowledge from baseline, after 12 weeks,
tetracycline. Sunscreens will need to be used with photosensitizers and applied mean improvement in knowledge was higher in the automated counseling group
as the first topical agent. than in the standard Website group. The automated counseling Website group
Regimens that may require more frequency of application may be difficult for rated their educational material more useful and more enjoyable to view than did
students or patients whose occupation limits flexibility. The frequency of the standard Website group. Internet-based patient education appears to be an
primary nonadherence to acne treatment has been characterized in terms of the effective method of improving acne knowledge among adolescents.193
complexity of multidrug acne regimens. Overall, 27% of patients did not fill all
their prescriptions; with one, two, or three or more treatments, 9%, 40%, and
31%, respectively, did not fill all their prescriptions. Authors concluded some Monitoring of the Pharmaceutical Care Plan
patients may not complete acne treatment because one or more of their Tables 113-2 to 113-4 provide a guide for monitoring patients with acne. Table
medications were never obtained. Primary adherence to an acne treatment 113-2 outlines individual drugs, their most common adverse effects, parameters
regimen is better when only one treatment is prescribed.190 History of poor to monitor, and issues to note. Table 113-3 outlines general effectiveness and
adherence because of intolerance of topical treatments may be countered by safety end points, monitoring parameters, and degree of change and time frames
reducing the strength of treatment, using a different preparation of the drug, or for short- and long-term outcomes. Table 113-4 is a guide for monitoring acne
switching to an alternative topical agent that causes less irritation. patients with consideration to the severity grading of acne types I through IV.
TABLE 113-3 Monitoring Therapy for Acne: Parameters and Frequency
EVALUATION OF THERAPEUTIC OUTCOMES
Provide a monitoring framework for patients with acne. Parameters should
be monitored by the patient and recorded in a diary. Therapy should be
appropriately tapered in response to improvement or resolution. The healthcare
professional should be responsible for ensuring that the treatment plan remains
on schedule and is effective with no adverse effects. The patient should be
contacted within 2 to 3 weeks to determine progress.
Acne is poorly understood by adolescents. These patients often lack
knowledge of the cause of the disorder and aggravating factors, indications for
self-care versus prescription treatment, expected onset of effect, sequence of the
healing process, duration of treatment, appropriate application of topical agents,
maximal achievable effects, expected adverse effects, safety concerns, and the
TABLE 113-4 Monitoring Care Plans for Acne Types I Through IV
CONCLUSION
Considerable gaps remain in the understanding of acne, despite all that is known
about the pathogenesis of acne and the mechanisms of effective drugs for
controlling its symptoms, progression, and complications at structural,
biochemical, and physiologic levels. It is still not possible to precisely define the
cause of one of the most common skin diseases, nor is it possible to identify a
cure for a condition that affects a very large proportion of the global population.
HGL high glycemic load
Postclass Engaged Learning Activity
IGF insulin-like growth factor
This activity is intended to build your self-assessment skills and your ability to MMPP mild-to-moderate papulopustular
critically evaluate key relevant information and/or misconceptions in the P. acnes Propionibacterium acnes
patient care process, as applied to a select patient scenario. After reflecting on
PAPA pyogenic arthritis, pyoderma gangrenosum, acne
what you have learned about clinical presentation of acne, triggers, patients at
risk, and guidelines about best practice therapy, create a small case scenario PBV pollen bee venom
followed by a series of multiple-choice questions and answers based on a PDT photodynamic therapy
patient with noninflammatory comedonal acne. In each lead-in question, try to QOL quality of life
test key elements such as essential decisions, common misconceptions or SAPHO synovitis, acne, pustulosis, hyperostosis, osteitis syndrome
errors. Lead-ins can address patient assessment, differential diagnosis, patient SPF sun protection factor
communication, investigations, drug therapy problem identification, risk
TTO time trade-off
factors, nonpharmacologic treatment, nonprescription treatment, prescription
treatment, referral or triage, or safety. Continue the case example with
sequential questions, changing the situation to provide further case details, REFERENCES
such as complications, altered circumstances, variations. You can also retest
with another variation (eg, a relative). Next, provide a second case and series 1. Cunliffe WJ, Gould DJ. Prevalence of facial acne vulgaris in late
of 5 to 6 questions, where the patient presents with mild-to-moderate adolescence and in adults. Br Med J. 1979;1:1109–1110.
inflammatory acne. Sequential questions can provide further circumstances, 2. Rademaker M, Garioch JJ, Simpson NB. Acne in schoolchildren: No
such as progressing to moderate or severe forms. Style tips: Use single best longer a concern for dermatologists. BMJ. 1989;298:1217–1219.
answer style (the distractors should have some element of truth to be attractive 3. Kilkenny M, Merlin K, Plunkett A, Marks R. The prevalence of common
to the test-taker, but not be the most appropriate response). Have one correct skin conditions in Australian school children, III: Acne vulgaris. Br J
answer with two distractors, or three if necessary: do not have five answer Dermatol. 1998;139:840–845.
options. Avoid true-or-false and all-or-none-of-the-above items, and keep
4. Nijsten T, Rombouts S, Lambert J. Acne is prevalent but use of its
options same length. Example: Which is the most relevant information to
treatments is infrequent among adolescents from the general population. J
interpret about this patient’s needs when eliciting the history of their signs and
Eur Acad Dermatolog Venereol. 2007;21:163–168.
symptoms? (List three choices, with one best answer.)
5. Bhate K, Williams HC. Epidemiology of acne vulgaris. Br J Dermatol.
2013;168(3):474–485.
ABBREVIATIONS 6. Smithard A, Glazebrook C, Williams HC. Acne prevalence, knowledge
about acne and psychological morbidity in mid-adolescence: A
BGA best guideline acne community-based study. Br J Dermatol. 2001;41:577–580.
CAM complementary and alternative medicine 7. Pandey SS. Epidemiology of acne vulgaris. Indian J Dermatol.
COC combination oral contraceptive 1983;28:109–110.
CRH corticotropin-releasing hormone 8. Kubba R, Bajaj AK, Thappa DM, et al. Acne in India: Guidelines for
management—IAA Consensus Document: Epidemiology of acne. Indian J
FDA Food and Drug Administration
Dermatol Venereol Leprol. 2009;75(suppl 1):S3.
GHQ general health quality
9. Shalita AR. Acne vulgaris: Pathogenesis and treatment. Cosmet Toiletries.
You might also like
- Acne in The Adult: A. Ascenso and H. Cabral MarquesNo ratings yetAcne in The Adult: A. Ascenso and H. Cabral Marques10 pages
- Acne Vulgaris: Audi Adibah - Affan Syafiqi - Amanina Nasir - Nurul Hidayu - Nik Nor Liyana - SathishwaranNo ratings yetAcne Vulgaris: Audi Adibah - Affan Syafiqi - Amanina Nasir - Nurul Hidayu - Nik Nor Liyana - Sathishwaran38 pages
- Acne Scars: Subcision: Methods and TechniquesNo ratings yetAcne Scars: Subcision: Methods and Techniques3 pages
- Isotretinoin for Non-Acne Skin ConditionsNo ratings yetIsotretinoin for Non-Acne Skin Conditions40 pages
- Acne Treatment Challenges - Recommendations ofNo ratings yetAcne Treatment Challenges - Recommendations of11 pages
- What Is Acne?: Propionibacterium Acnes, or P. Acnes) Begin To Grow Inside TheNo ratings yetWhat Is Acne?: Propionibacterium Acnes, or P. Acnes) Begin To Grow Inside The6 pages
- Update On The Management of Rosacea From The American Acne & Rosacea SocietyNo ratings yetUpdate On The Management of Rosacea From The American Acne & Rosacea Society8 pages
- Androgens in Women: Androgen-Mediated Skin Disease and Patient EvaluationNo ratings yetAndrogens in Women: Androgen-Mediated Skin Disease and Patient Evaluation10 pages
- Melasma Treatment - A Complete Guide To Clearer Skin - Devriz HealthcareNo ratings yetMelasma Treatment - A Complete Guide To Clearer Skin - Devriz Healthcare10 pages
- Atlas of Trichoscopy Dermoscopy in Hair and Scalp Disease - 1st Edition Reference Book DownloadNo ratings yetAtlas of Trichoscopy Dermoscopy in Hair and Scalp Disease - 1st Edition Reference Book Download17 pages
- Psychosocial Aspects of Aging Skin - 2005 - Dermatologic ClinicsNo ratings yetPsychosocial Aspects of Aging Skin - 2005 - Dermatologic Clinics6 pages
- Radiofrequency Review of Literature 2019No ratings yetRadiofrequency Review of Literature 201911 pages
- Micro-Plasma RF for Post-Burn HyperpigmentationNo ratings yetMicro-Plasma RF for Post-Burn Hyperpigmentation5 pages
- Permanent Hair Removal with ElectrolysisNo ratings yetPermanent Hair Removal with Electrolysis3 pages
- Carbon Peeling Laser Treatment To Improve Skin TexNo ratings yetCarbon Peeling Laser Treatment To Improve Skin Tex4 pages
- By Drafshan Mughal Resident Dermatology Chk/DuhsNo ratings yetBy Drafshan Mughal Resident Dermatology Chk/Duhs76 pages
- Treatment of Melasma by Low - Uence 1064 NM Q-Switched Nd:YAG LaserNo ratings yetTreatment of Melasma by Low - Uence 1064 NM Q-Switched Nd:YAG Laser6 pages
- Ae Licensees Procedural Service Determinations - 03.2025No ratings yetAe Licensees Procedural Service Determinations - 03.20256 pages
- MEDIFINE Beginners & Advanced Facial Courses 2021No ratings yetMEDIFINE Beginners & Advanced Facial Courses 20215 pages