PHYSICAL ASSESSMENT
Physical Assessment is an organized, systematic process of collecting
objective data based on health history and head-to-toe examination. The physical
assessment is the step in the nursing process. It provides the foundation of the nursing
care plan in which your observations play an integral part in the assessment,
intervention, and evaluation phases (Brookside Associates, 2015). Thorough
assessments are made with the client's complaints; the nurse's observation of
problems, the client's presenting problem, nursing interventions provided, and medical
therapies.
The techniques used in assessment include inspection, palpation, percussion,
and auscultation. Inspection is the visual examination of the client. This includes the
observation of the color, size, location, movement, texture, symmetry, odors, and sound
as you assess each body system. Palpation is the use of the hand to touch to determine
temperature, moisture, size, shape, position, texture, consistency, and movement. This
can have two types: light palpation and deep palpation. Percussion is the string of the
body surface with short, sharp strikes to produce palpable vibrations and characteristic
sounds. Auscultation listening to sounds produced inside the body. This includes breath
sounds, heart sounds, vascular sounds, and bowel sounds with a stethoscope.
The physical assessment was done on February 23, 2023, at 8:00 PM, 1 day
post-operative at Manuel J. Santos Hospital. In performing the procedure, student
nurses considered the patient's age and feelings, beliefs, understanding, and privacy
while providing appropriate control measures and safety precautions. Different
instruments such as stethoscopes, thermometers, blood pressure apparatus, penlight,
and watches are essential tools to efficiently determine the overall state of health and
further assess the physical condition of the patient to create a client-centered nursing
care plan.
General Assessment
Patient D’s latest vital signs during the last day of the physical assessment were
as follows: BP- 100/80, PR- 64 bpm, RR- 20 cpm, Temperature- 36.4C, and O2
Saturation- 99%. Patient C was oriented and the train of thought was coherent and
logical. Upon a quick observation of Patient C emphasized pain around the incision
part upon the assessment with a scale of 7/10. The dressing was observed around
the abdomen from the operation. Fullness (bloating) in the abdomen was also noted.
Can tolerate standing and walking around the room. Moreover, he can able to
perform a range of motion exercises like flexion and extension. No alteration in gait
was observed. The patient was responsive and can talk freely with the student
nurses.
Legend:
BLACK – NORMAL OBSERVATION
RED – ABNORMAL OBSERVATION
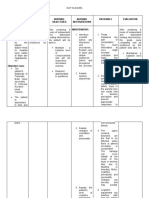
SYSTEM INSPECTION PALPATION PERCUSSION AUSCULTATION
Scalp and Hair is black and no Hair is soft N/A N/A
Hair presence of and shiny
dandruff. with no
presence of
nodules and
tenderness.
Head and The head is Has a round N/A N/A
Face normocephalic with and smooth
symmetrical facial skull contour.
features. He can
slightly bend his
neck.
Skin The complexion is The patient’s N/A N/A
light brown. No skin is soft.
presence of wounds Afebrile when
was observed. No the skin was
presence of palpated.
jaundice can be
observed. Skin turgor is
1 second.
Eyes and Eyebrows are Intact blink N/A N/A
Visual symmetrically reflex
Acuity aligned. Eyelashes
curl out and are
evenly distributed.
Iris were dark
brown, with pupils
equal in size, and
does dilate when
reacting to light. Can
follow light
accommodation.
Jaundice was not
noted in both eyes.
Ears and Auricles have the The external N/A N/A
Hearing same color as facial ear is soft
skin. The ears are and firm.
symmetrical. No Pinna recoils
presence of immediately
yellowish cerumen when folded.
was noted.
Nose and The nasal septum No presence N/A N/A
Sinuses and midline were of any
intact. Left and right nodules,
nares are polyps or
symmetric. masses on
nose. No
tenderness
Mouth and The lips and the No N/A N/A
Throat mouth were pink. tenderness or
No cavities were masses. Able
noted on both the to elicit gag
upper and lower reflex
portion. Palates and
mucus membranes
were pink. The
tongue is pink. No
whitish discoloration
can be seen.
Input: 1,035 mL
Neck Skin color is light The carotid N/A N/A
brown like other pulse is
parts of the body. palpable.
Able to move neck Lymph nodes
in different are not
directions. inflamed. No
deviation of
the trachea is
noted. The
thyroid gland
is at the
midline, firm,
and non-
tender.
Thorax Symmetrical chest The pain was Upon Adventitious
and Lungs expansion. Skin is felt by the percussion, a sounds are not
intact. The spine is patient upon resonating heard upon
vertically aligned. light palpation sound was auscultation.
The respiratory rate (around the heard on both
was 20 breaths per incision part). posterior
minute. aspects of the
lungs.
Heart and Jugular veins were Pulses were N/A The patient had
Central not visible and no palpable on a heart rate of
Vessels distention was the carotid 64 beats per
noted. pulse with a minute upon
relatively auscultating the
smooth rapid apical pulse. No
upstroke. murmurs were
heard.
Breast and Breasts were No N/A N/A
Axillae symmetrical. Skin tenderness
is uniform in color and enlarged
(same appearance nodules were
in appearance as felt upon
the skin of the palpation.
abdomen). No
discharges, lesions,
or discoloration
were noted. The
nipple is brownish.
Axillary body
temperature is
36.4C
Upper Smooth in texture, Capillary refill N/A N/A
extremities nails are clean and at 2 seconds.
trimmed. No Radial and
presence of scars Brachial
or wounds was pulse
seen. palpable.
Abdomen Skin is light brown Bowel sounds Generalized Pain was felt
as the other parts of were audibly tympany over upon light
the body. The ranging from bowel. palpation on the
abdominal contour bowel sounds umbilicus area
(Assessed is flat, globular, and per minute. (incision part).
through symmetrical. Its
movements are also
IAPePa) symmetrical. The
dressing was noted
around the
abdomen from the
operation. Fullness
(bloating) of the
abdomen was
noted.
The patient declined
Genitals to let his genitals be N/A N/A N/A
and Anus assessed.
Urinates five times a
day.
Input: 1,035 mL &
Output: 850 mL
Defecates twice a
day.
Lower Skin is light brown Skin turgor is N/A N/A
extremities on the areas 2 seconds.
exposed to sunlight. No pain was
The toenails were felt when
clean and trimmed. palpating the
feet.
MUSCULOSKELETAL RESULT
SYSTEM
MOTOR FUNCTION
A. GROSS The patient can raise his hand without difficulty and
can also perform a range of motion exercises as
evidenced by flexion and extension.
B. FINE The patient can write on the paper. He can also fold
the paper without difficulty.
C. LANGUAGE The patient’s speech was clear and his voice was
loud enough to be heard when answering the set of
questions being asked. The patient was responsive
and can talk freely with the student nurses.
Patient J can tolerate sitting and standing on his own.
D. GAIT No alteration in gait was observed.
NEUROLOGIC
FUNCTION
BEHAVIOR The patient is coherent; oriented to people, time,
place, and situation.