
SNC Module 19 - Quality Management - Revised Oct 16
SNC Module 19 - Quality Management - Revised Oct 16
Uploaded by
Yza WagayenCopyright:
Available Formats
SNC Module 19 - Quality Management - Revised Oct 16
SNC Module 19 - Quality Management - Revised Oct 16
Uploaded by
Yza WagayenOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Copyright:
Available Formats
SNC Module 19 - Quality Management - Revised Oct 16
SNC Module 19 - Quality Management - Revised Oct 16
Uploaded by
Yza WagayenCopyright:
Available Formats
STROKE NURSE
CERTIFICATION
Module 19
Quality Management
Autho r:
Dr. Thomas Luiz, Dieter Lerner
DENIT at Fraunhofer IESE, Kaiserslautern
U pdated by:
Gilbert Steinfurth
2016
CONTENTS
PA GE
1 Introduction to Quality Management in Healthcare 3
1.1 History of quality management in healthcare 4
1.2 Integration of industrial methods of quality management 5
2 Industrial Models of Quality Management 5
2.1 The Plan, Do Check, Act (PDCA) model 5
2.2 Total Quality Management (TQM) 5
2.3 Continuous quality improvement 8
3 Quality Improvement Strategies 10
3.1 Introduction 10
3.2 Interdisciplinary checklists: simple but effective. 10
3.3 Crew resource management. 11
3.4 Standards of care 11
4 Measuring Quality 12
4.1 Quality metrics in a neurocritical ICU 12
4.2 Quality metrics in stroke registers 13
4.3 Measuring and managing outcomes 13
5 Benchmarking 15
6 Risk Management 16
7 Quality Improvement through Dedicated Units 18
7.1 Introduction to neurocritical care as a subspecialty 18
of critical care medicine
7.2 Does neurocritical care expertise make a difference? 18
7.3 Does organised stroke unit care make a difference? 18
8 Leadership and Management Implications 20
9 Test Yourself 22
10 Literature 26
11 Appendix 28
Stroke Nurse Certificate: Module 19 2
Quality Management
1 INTRODUCTION TO QUALITY MANAGEMENT IN HEALTH CARE
1.1 HISTO RY O F Q UALITY M ANAGEM ENT IN HEALTHCARE 1
The quality of healthcare has been a major problem in many countries for over a
century. Finding a definition, methods of evaluation, monitoring and quality
improvement have been key issues for both researchers and healthcare professionals.
Donabedian noted in 1966 that the quality of healthcare is a “remarkably difficult notion
to define”2. He developed the initial theoretical model postulating that quality can be
measured using three categories: structure, process and outcome3. This model is the
most widely referenced model of quality in healthcare.
The motivation for a systematic quality evaluation of healthcare was primarily of a
professional nature. The Hippocratic Oath and the work of Ignaz Semmelweis and
Florence Nightingale serve as examples of professional motivation for a systematic
quality evaluation and improvement in healthcare.
Table 1 provides a historical overview of quality initiatives in the history of the
healthcare system.
TABLE 1: HISTO RICAL VIEW OF QUALITY INITIATIVES AND QUALITY
4
METHODS IN HEALTHCARE
PERIOD INITIATIVES / METHODS (SELECTION)
• Physician licensing
UP TO 1900 • Specialty societies
• Individual efforts
• Professional certification
1900–1920 • Legislation
• Nursing and hospital standardisation
• Studies on nursing conduct
1920–1940 • Health insurance legislation
• Government legislation and standards
• Professional standards
1940–1980 • Accreditation of hospitals
• Rapid increase in literature
• Increase in published standards
• Publications on quality indicators
1980–2000
• Government involvement raised
• Evidence-based medicine Movement
• Integration of industrial methods of quality management (TQM,
quality circles)
• New international standards (e.g. ISO 9000/9001)
2000-BEYOND
• Evidence-based Practice / Best Practice Movement
• Evidence-based Dissemination and Implementation research
• Benchmarking
Stroke Nurse Certificate: Module 19 3
Quality Management
1.2 INTEGRATION OF INDUSTRIAL M ETHODS OF QUALITY M ANAGEM ENT
In recent years, industrial models have influenced the way quality is currently
understood and measured in healthcare settings. Industry leaders who have influenced
the understanding of healthcare quality include (for example) Walter Shewhart, Joseph
Juran, Philip Crosby, and W. Edwards Deming. These leaders provided blueprints from
which healthcare quality management approaches have been derived.
In this chapter, the following concepts are explained: The Plan, Do Check, Act (PDCA)
model, Total quality management (TQM), continuous quality improvement, standards,
outcomes management, and risk management.
Stroke Nurse Certificate: Module 19 4
Quality Management
2 INDUSTRIAL MODELS OF QUALITY MANAGEMENT
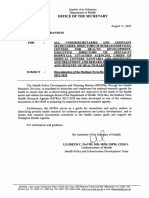
2.1 THE PLAN, DO CHECK, ACT (PDCA) M O DEL5
Shewhart explored causes of variation in industrial work processes. He evaluated these
variations and developed a model to improve work processes. Deming adapted his
work and refined the model (see Fig. 1).
Plan: identify an issue and plan a process improvement
Do: implement the process improvement
Check: Check the results of the new process
Act: Based on the analysed data propose and implement a refined process
PLAN
AC T DO
C HE C
K
Figure 1: PDCA Cycle
2.2 TO TAL Q UALITY M ANAGEM ENT (TQ M ) 6
TQM is a management philosophy that emphasises a commitment to excellence
throughout the organisation. TQM was adopted by the Japanese and helped transform
their industrial development after World War II. The principles of TQM are now widely
used to improve quality and customer satisfaction in a number of service industries,
including healthcare. Four core principles of TQM can be distinguished: customer/client
focus, total organisational involvement, use of quality tools and statistics for
measurement and identification of key processes for improvement.
Stroke Nurse Certificate: Module 19 5
Quality Management
C O RE PRINC IPLE S OF TQ M: C LIE NT FO C U S, T OTAL O RGANI SATIO NAL
INVO LVE ME NT, USE O F QU ALITY T OO LS FO R M EASU REM ENT ,
ID ENTI FICAT IO N O F K E Y PRO C ESSE S
2.2.1 Customer/Client Focus
A fundamental aspect of quality management is to address the needs of both internal
and external customers. Internal customers include employees and departments within
the organisation such as the laboratory, admitting office and environmental services.
External customers of a healthcare organisation include patients, visitors, referring
physicians, emergency medical services, insurance companies and regulatory agencies
such as the Joint Commission, which accredits healthcare organisations and public
health departments.
2.2.2 Total organisational involvement
The goal of quality management is to involve all employees and empower them with
the responsibility to make a difference in the quality of service they provide. This
means all employees must have knowledge of the TQM philosophy as it relates to their
job and the overall goals and mission of the organisation.
2.2.3 Use of quality tools and statistics for measurement
A common management adage is: “You can’t manage what you can’t measure.” There
are many tools, formats and designs that can be used to build knowledge, make
decisions and improve quality. Tools for data analysis and display can be used to
identify areas for process and quality improvement and to then benchmark the
progress of improvements. Deming applied the scientific method to the concept of
TQM to develop a model he called the PDCA cycle (see above).
2.2.4 Identification of key processes for improvement
All activities performed in an organisation can be described in terms of processes.
Processes within a healthcare setting can be:
• Systems-related (e.g. admitting, discharging and transferring patients)
• Clinical (e.g. administering medications, managing pain)
• Managerial (e.g. risk management and performance evaluation)
Processes can be very complex and involve multidisciplinary or interdepartmental
actions. Processes involving multiple departments must be investigated in detail by
members of each department involved in the activity so that they can proactively seek
opportunities to reduce waste and inefficiencies and develop a way to improve
performance and promote positive outcomes.
A typical example is the case of a 68 year old patient with a TIA. Ultrasound reveals a
severe stenosis of the internal carotid artery. The question of urgent carotid surgery
arises. The patient is multimorbid, presenting with coronary artery disease, ischemic
cardiomyopathy, hypertension and chronic hepatic failure. Within one day, the
following preparations have to be arranged: Neurologist: clinical and ultrasonographic
examination.
Neuroradiologist: performance of angiographic imaging study.
Vascular surgeon: indication of surgery
Anaesthetist and cardiologist: assessment of perioperative cardiovascular risk
Stroke Nurse Certificate: Module 19 6
Quality Management
Hepatologist: assessment of the hepatic function
Surgery management: planning of operating room resources
2.2.5 EFQM ® Model for Business Excellence 7
The EFQM® model is a quality management system adopting the principles of TQM
developed in 1988 by the European Foundation for Quality Management. It aims to
involve all employees in a continuing improvement and learning processes. The model
was refined in 2003 and again in 2010. An important element of EFQM® is the periodic
self-assessment of the organisation.
The EFQM excellence model is based on nine criteria, grouped into two parts: five
enabler criteria (Leadership, Policy and Strategy, Employees, Resources and
partnerships, Processes and Services) and four results criteria (Customer results,
Employee results, Society results, Business results). There is a dynamic relationship
between the enablers and the results, as excellence in the enablers will be visible in the
results.
®
Figure 2. The EFQM model of excellence
E FQ M a s an examp le of a
To tal Qua lity M ana gement Mo del
An organisation using the scoring profile of the EFQM excellence model can earn up to
1,000 points distributed among the nine categories (see Figure 2).
RADAR, a method of evaluation, is central to the excellence model. It comprises four
elements: Results, Approach, Deployment, Assessment and Review. In order to fulfil
the RADAR logic, an organisation needs to:
• Determine the results it is aiming for (assessment considers trends, targets,
comparisons, causes and scope);
• Plan and develop an integrated set of sound approaches to attain the results;
• Deploy approaches in a systematic way;
• Assess and review the approaches by monitoring and analysing the results
achieved.
The EFQM excellence model does not prescribe what to do and how to do it; rather, it
provides a framework to enable individual organisations to assess themselves and look
for opportunities to improve their service. For this to be successful, self-assessment
must not be seen as a form of accusation and “blame”, but rather as a tool for
Stroke Nurse Certificate: Module 19 7
Quality Management
systematic improvement. Improvements can only be made once areas for
improvement have been identified and this follows on from an open and honest self-
assessment.
There are a number of approaches for undertaking self-assessment, for example, using
matrix charts, workshops, questionnaires, peer involvement or award simulation. For
quality management to be effective, every level of the organisation must know what
the aims are and how they are to be achieved. After this awareness for quality
problems has been created, it is necessary to train quality owners. They, in turn, are
responsible for the self-assessment of their particular criteria. An outcome report is the
result of the self-assessment and this, in turn, can be discussed with treatment
receivers, funders and any other groups involved in healthcare.
External-Assessment
Once consensus regarding the outcome report has been attained within the
organisation, a copy of the report is sent to an external assessor. The external assessor
evaluates the organisation using the RADAR scheme.
Excellent organisations (e.g. hospitals) are successful by:
• Achieving well-balanced business results in order to satisfy and even exceed
stakeholders’ expectations
• Enhancing customer value, e.g. improved neurologic status after stroke unit
therapy
• Leading with vision, inspiration and integrity
• Managing processes and making decisions based on facts, e.g. analysing door-
needle times or complication rates
• Building up a culture of respect and responsibility for the staff members, e.g.
integration of physically disabled employees
• Fostering innovation and creativity of their stakeholders, e.g. by introducing a
company suggestions scheme
• Building up and preserving trustful relationships and partnerships, e.g. with the
EMS system and rehabilitation facilities
• Accepting responsibility for a sustainable economic, social and ecologic
• Future, e.g. digital archiving of documents and x-ray images to reduce paper
consumption and to reduce exhaust emissions
C O NTINU OU S QU ALITY IM PRO VE ME NT I S A NEVE R- E NDING
E NDE AVO R
TO A CH IE VE EXC E LLENC E
2.3 CO NTINUO US Q UALITY IM PRO VEM ENT 8
TQM is the overall philosophy, whereas continuous quality improvement (CQI) is the
process used to improve quality and performance. In healthcare organisations, CQI is
the process used to systematically investigate ways to improve patient care. As the
name implies, continuous quality improvement is a never-ending endeavour. It means
more than just meeting standards and thresholds or solving problems. It involves
evaluation, actions, strategies and a mind-set to strive constantly for excellence (see
Figure 3).
Stroke Nurse Certificate: Module 19 8
Quality Management
Figure 3: Continuous quality improvement
Accor ding to Law so n et al., the fo cus of q uality im pro vem en t initia tiv es
in a neuro critical car e unit s hould be f ocus ed on sev era l key a reas 9 :
1. D evelop ment and ad herence t o st anda rdis ed ev idence- ba sed
pr actices for pr event ing ho sp ital- acq uir ed conditio ns and
empha sis o n p atient s afety;
2. Regular r eview of q uality metrics , part icularly data , t o id entify
ar eas in need o f impr ov ement; a nd
3. D evelop ment of q uality pro ject s and initiat iv es t o corr ect.
Stroke Nurse Certificate: Module 19 9
Quality Management
3 QUALITY IMPROVEMENT STRATEGIES
3.1 INTRODUCTION
There is extensive literature on the effectiveness of various strategies to improve
quality and performance in the healthcare organisation, for example, in critical care
units (see Table 2).
TABLE 2: Q UALITY IM PRO VEM ENT STRATEGIES 10
STRATEGY DESCRIPTION
11 Packaging established and related interventions together in order
Bundles
to facilitate retention and implementation
Structured orders that allow non-physician clinicians to titrate
Protocols
therapies according to specified criteria
Reminder list to be reviewed prior to a procedure or on daily
Checklists
rounds.
Crew Resource
Using the collective intelligence and ability of the team.
Management
Periodic assessment and distribution of quality measures to clinical
Audit and feedback
team
Using advertising tools (posters, emails) to disseminate
Social marketing
information and provide encouragement to change behavior.
Opinion leader,
Engaging high-impact, well-respected individuals to influence their
academic detailing,
peers
continuing education
3.2 INTERDISCIPLINARY CHECKLISTS: SIM PLE BUT EFFECTIVE.
At its most simple form, a checklist can be thought of as memory aid to help someone
to be sure not to omit a key step in a procedure. The World Health Organisation’s
search for a way to decrease operative mortality worldwide that could be implemented
in a simple way resulted in the Surgical Safety Checklist, which serves both as a safety
tool and as a team-orienting exercise based on the crew resource management
approach (see below). In their worldwide study, Haynes and his colleagues found that
implementation of the checklist was associated with a reduction in rate of death from
1.5 % to 0.8 %.12
Checklists are valuable in the stroke unit as well. Drawing on an example of Weiss and
colleagues, they could show that the implementation of an ICU-rounding checklist was
associated with a 48% reduction in ICU mortality.13 These results show that breaking
down a task into its component parts and standardising the approach can decrease
unnecessary variability and thereby improve outcomes.
Stroke Nurse Certificate: Module 19 10
Quality Management
3.3 CREW RESO URCE M ANAGEM ENT
A further strategy is to focus on the dynamic of the care team. Crew resource
management is the term that is used to describe the process by which the collective
intelligence and ability of the group can exceed that of its component individuals.
Because a high-functioning team is critical to mishap prevention, crew resource
management works to decrease the “power distance” and, in so doing, improve
information transfer.14
3.4 STANDARDS O F CARE 15
3.4.1 Definitions
According to Sullivan and Decker, standards are written statements that define a level
of performance or a set of conditions determined to be acceptable by some authorities.
In the opinion of Marquis, a standard is a predetermined level of excellence that serves
as a guide for practice.16
Standards can relate to three major dimensions of quality care (known as Donabedian’s
model or framework; see above): structure, process and outcome. Donabedian’s
framework is useful to understand the relationships between outcomes and the
structure and processes that have produced them.
• Structure standards relate to the physical environment, organisation or
qualification of staff.
• Process standards are those related to the actual delivery of care.
• Outcome standards involve the end results of care that have been given. Within
these dimensions, measuring and managing outcomes are especially important.
3.4.2 Organisational Standards vs. Evidence-Based Guidelines
Each organisation and profession must set standards and objectives to guide individual
practitioners in performing safe and effective care. We distinguish between
organisational standards and evidence-based guidelines developed and published from
scientific associations.
Organisational standards outline levels of acceptable practice within the institution.
Each organisation will set out its specific standards in a policy and procedures manual.
O RGANI SATIO NAL S TANDARD S SHO U LD SP EC IFY E VID ENC E -B ASE D
STAND ARD S FRO M SC IE NTIFIC ASS OC IAT IONS .
Evidence-based guidelines, such as those developed by the AHA/ASA17 or ESO18, are
developed following an extensive review of the scientific literature and suggest what
interventions will likely lead to the best possible patient outcomes. In other words,
clinical practice guidelines are based on current research findings and best practices
(see module Evidence-based Nursing).
Stroke Nurse Certificate: Module 19 11
Quality Management
4 MEASURING QUALITY
4.1 Q UALITY M ETRICS IN A NEURO CRITICAL ICU
To improve the quality of care, performance must be measured. Controversy exists
regarding whether quality measures should be interventions (process or structural) or
outcome measures. Process measures are easier to measure than outcome measures
and can be used to provide immediate feedback to providers regarding their
performance.
Outcome measures are, ultimately, what patients care about (see below). It is
important to select quality measures in which evidence regarding the association
between the intervention (structure, process) and outcome is strong. Table 3 gives an
overview of possible quality measures and their definitions.
TABLE 3: Q UALITY M EASURES AND DEFINITIO NS 19
STRUCTURAL MEASURES
DEFINITION
/ ACCESS MEASURES
20
Rate of delayed admissions to the SU
Rate of delayed admissions 21
or NCU
Number of cancelled OR cases owing to lack
Cancelled organisational resources (OR)
of CT, SU/NICU bed or available staff
Number of delay discharges from SU or NCU
Rate of delayed discharges due to lack of beds in step down units or
rehabilitation units
PROCESS MEASURES DEFINITION
The percent of days on which patient
Appropriate use of prophylaxis interventions
received prophylaxis (e.g. against aspiration)
The percentage of rtPA-treatment in patients
Appropriate use of medications with ischemic stroke, admitted within the 3h
time window
The percentage of deviations from treatment
protocols without justifications (e.g., patients
Deviations from the organisational
not on continuous ECG monitoring; patients
procedures (treatment protocols)
receiving rtPA despite absolute
contraindications)
OUTCOME MEASURES DEFINITION
The percentage of patients with dysphagia
Rate of dysphagia-associated aspirations
and aspiration or aspiration- pneumonia over
or pneumonias
1.000 admissions
Rate of catheter-related Rate of catheter-related bloodstream
bloodstream infections infections per 1,000 catheter days
Percentage of patients with an unexpected
Cardiac arrest rate
cardiac arrest over 1,000 admissions
% of SU / NCU discharges who die
SU and NCU mortality rate
in the SU / NCU
Average SU / NCU Length of stay (LOS) Average LOS
Excellent neurologic status at discharge Percentage of patients with a modified
from hospital Ranking scale of 0 or 1
Stroke Nurse Certificate: Module 19 12
Quality Management
TM22
Patient / family satisfaction Quality of life assessment (e.g. EQ- 5D )
Performance and outcomes are measured or quantified by
indicators
4.2 Q UALITY M ETRICS IN STRO KE REGISTERS
There are many international organisations involved in quality measurement for acute
stroke, and a complex landscape of quality measures exist.23 In this chapter, we
provide the example of the German Stroke Registers Study Group. Since 1994, a
number of regional stroke registers have been established for the purpose of external
quality assurance in acute inpatient stroke treatment. Since 1999, these regional
registers have been collaborating within the framework of the Arbeitsgemeinschaft
Deutscher Schlaganfall-Register (ADSR, German Stroke Registers Study Group).24
The ADSR was established in order to standardise the collection of data in the area of
acute hospital stroke care and to develop consistent, standardised quality indicators.
Additionally, data from the participating registers are pooled regularly and jointly
scientifically evaluated. Currently, a set of 19 evidence-based indicators is being used
to monitor the quality of stroke care in the participating hospitals (see Appendix).
4.3 M EASURING AND M ANAGING O UTCO M ES 25
4.3.1 Outcome
An outcome is the result or results obtained from the efforts to accomplish a goal. The
term “outcomes” has also been defined as the conditions in patients and others that
healthcare delivery aims to achieve. Donabedian described outcomes as changes in the
actual or potential health status of individuals, groups or communities.26
4.3.2 Indicators
Indicators are valid and reliable measures related to performance or outcome. They are
the specific tools used to make quality visible to stakeholders in health care. Outcomes
are measured or quantified by observing or describing indicators.
The choice of appropriate indicators is critical for the acceptance and efficiency of a
quality management system. A good indicator should, therefore, provide a realistic
insight into the state of stroke management provided in a participating institution.
Usually, quality indicators are the result of a multi-phase consensus process performed
by a group of experts in the field (e.g. achieved by means of the Delphi Method). The
duration of validity should be limited (e.g. to 3 years), to ensure the indicator’s validity.
4.3.3 Attributes of a Good Quality Indicator: RUMBA-Rule
TABLE 4: ATTRIBUTES OF A GOOD QUALITY INDICATOR
CHALLENGE DESCRIPTION AND EXAM PLE
Stroke Nurse Certificate: Module 19 13
Quality Management
The chosen indicator must be of high relevance to the
Relevant selected problem, (e.g. the rate of aspiration pneumonia,
a complication associated with high mortality).
Healthcare providers must easily recognise the indicator
Understandable
and its impact.
The indicator must be measurable with a high grade of
Measurable
reliability and validity.
The indicator is basically susceptible to quality
improvement efforts based on behavioral modification,
Behaviourable
e.g. systematic dysphagia screening and swallow
training.
Significant improvements must be achievable in daily
Achievable practice by reasonable expenditure (e.g. dysphagia
screening takes only a short time).
4.3.4 Outcom es M anagem ent
Outcomes management is a new method in which costs and quality are concurrently
and retrospectively measured and evaluated in order to improve clinical practice.
Internal or external data from outcomes research or other healthcare providers are
used as benchmarks against which process, quality, and financial goals can be set and
achieved. Additionally, data from internal clinical information systems can be used to
provide a linear view of patient care delivery and associated costs.
B ENC HMA RK IN G: CO M PAR ING O NE SELF W ITH T HE B EST INSTITUTIO NS A ND
UNDE RS TAND ING THE R EA SO NS FO R THE IR SUC CESS .
4.3.5 Outcomes Research
Outcomes research is a field in health services research that examines improvements in
functional status and quality of life. What makes outcomes research distinct from the
vast bodies of research that examine endpoints in patients (i.e. mostly clinically
oriented research) is that outcomes researchers seek to differentiate the various factors
that influence the outcomes (e.g. patient-level or system-level factors).
Outcomes researchers are especially concerned about understanding “real life”
differences between expected and observed outcomes and between outcomes on
different units, in different institutions or at different points in time.
Outcomes are influenced by a number of factors – the specific treatment delivered is
only one factor. The factors influencing outcomes can be summarised and expressed in
the form of a mathematical “function” as follows:
O UTCO M ES = F (PA TIENT C LINIC AL C HAR ACT ER ISTICS AND R IS K F ACT O RS,
PA TIE NT DEM O GR APHICS, O R GANISA TIO N AL CHA RA CTE RISTICS
O F THE SE TTING, TR EATM EN T, RA NDO M C HAN CE)
Stroke Nurse Certificate: Module 19 14
Quality Management
5 BENCHMARKING 28
Many healthcare organisations and regulatory bodies have begun using benchmarking,
the process of measuring products, practices, and services, against best-performing
organisations as a tool for identifying desired standards of organisational performance.
In doing so, organisations can determine how and why their performance differs from
these exemplar organisations and use them as role models for standards development
and performance improvement.
For example, a hospital may look at its average “door-to-needle” times in acute
ischemic stroke, compare it to “door-to-needle” times of similar competitor facilities
and set a goal of decreasing the average “door-to-needle” times. The end goal is not to
mimic the practices of other institutions. Instead, it is to understand why their
processes are more effective. Only by understanding the reasons and processes
behind a competing hospital’s effectiveness will a benchmarking hospital be able to
develop a plan to improve their own processes. Benchmarking, however, is not an easy
exercise. Perhaps the most challenging aspect is that it needs to be an ongoing
approach, rather than a one-time initiative.
Continuous collection of data surrounding competing hospitals can be difficult because
most hospitals do not report their statistics publicly. However, the trend toward
greater transparency in the healthcare systems is slowly making benchmarking data
more readily available.
Stroke Nurse Certificate: Module 19 15
Quality Management
6 RISK MANAGEMENT 29
R ISK MA NAG EM ENT A IM S TO IDENT IF Y A ND AN ALYS E PO TE NTIAL R ISK S AN D
TO M IN IM ISE THE FR EQ UE NCY AND SE VE RITY O F UN PLAN NED A DV ERS E
EV EN TS.
Risk management is a component of quality management. Its purpose is to identify,
analyse and evaluate risks and then to develop a plan for reducing the frequency and
severity of accidents and injuries. Risk management is a continuous program of
detection, education and intervention. Risk management involves all departments of
the organisation. It must be an organisation-wide programme, which includes:
• Identification of potential risks for accident, injury, or financial loss.
• Reviews of current organisation-wide monitoring systems (e.g. incident reports,
audits, oral complaints, patient questionnaires).
• Analyses of the frequency, severity and causes of general and specific
categories of incidents that lead to injury or adverse outcomes for patients.
• Reviews and appraisals of safety and risk aspects of patient care procedures
and new programmes.
• Monitoring of laws and codes related to patient safety, consent and care.
• Identification of needs of patients and families
• Identification of educational needs and implementation via an appropriate
educational program.
• Evaluation of the results of the risk management program.
• Provision of periodic reports to administration, medical staff and board of
directors.
The implementation of a critical incident reporting system (CIRS) is a key element of
risk management. A CIRS is an anonymous (usually web-based) vigilance system
reporting unplanned critical incidents and near-miss events (unplanned events that did
not cause harm, but had the potential to do so). The purpose of a CIRS is to enhance
patient safety. This approach was first implemented in aviation and in industrial
processes.
Since the late 1990s, CIRS has gained increasing attention and acceptance in medicine,
especially in high-risk areas, e.g. emergency medicine, critical care medicine and
anaesthesiology. CIRS aim to improve the error culture. Therefore, it does not focus
on the individual person reporting a near-miss event or a potentially harmful mistake,
but on the circumstances that led to the event. The ultimate goal is to improve the
system (i.e. structures and processes) in a way that prevents future similar events,
especially real “disasters”. A CIRS must be actively “managed”, i.e. incoming reports
must be reviewed and responded to in a timely manner.
CIR S AIM TO IMP RO V E E RR O R CU LTURE AN D CO NSE CUTIV ELY P ATIENT
SAFE TY
Example: A CIRS report referred to mistaken coagulation lab results in a patient
receiving rt-PA for ischemic stroke. The neurologist erroneously received the lab results
of another patient. The mistake was not revealed until after the drug had been
administered. Fortunately, the patient undergoing fibrinolysis had a normal coagulation
test and no bleeding occurred. At that time, the reason for the mistake could not be
identified. Two days later, a second report referring to a similar scenario occurred.
Stroke Nurse Certificate: Module 19 16
Quality Management
On this occasion, the mistake was, fortuitously, recognised by the neurologist before
rt-PA was administered. (That patient, in fact, suffered from severe thrombocytopenia.)
Based on additional information derived from the second report, the CIRS leader was able
to identify the underlying cause: new patient labels with inadequate adherence to the
specimen tubes. Consequently, all personnel were alarmed about this problem, additional
safety advice was provided and new adhesive labels were introduced as soon as possible.
Stroke Nurse Certificate: Module 19 17
Quality Management
7 QUALITY IMPROVEMENT THROUGH DEDICATED UNITS
7.1 INTRODUCTION IN NEURO CRITICAL CARE AS A SUBSPECIALTY O F
CRITICAL CARE M EDICINE
Intensive care medicine is the science and the art of detecting and managing critically
ill patients while preventing further deterioration, in order to achieve the best possible
outcomes. Intensive care medicine emerged as a specialty in the 1950s with its origins
in Copenhagen during the poliomyelitis epidemic, where patients with respiratory
failure were artificially ventilated.30
However, Walter Dandy, a neurosurgeon, established in the 1920s two adjacent two-
bed rooms that served as a neurosurgical ICU and the first intensive care unit (ICU) at
the Johns Hopkins Hospital in Baltimore, Maryland.31 In the 1970s, stroke units began to
appear that were dedicated to the care of stroke patients and are some of the direct
precursors to modern neurocritical care units.
Advances in anaesthesiology for neurosurgery also generated a need for specialised
postoperative care units. In the 1980s and 1990s, research in neurology and
neurosurgery began to take root, leading to improved diagnosis and therapy, and
prompting the inception of the first specialised neurocritical care units.32
The backbone of the neurointensive care unit is the nursing staff. Nurses in these units
not only master the general skills needed in intensive care medicine, but they are
proficient in the detailed neurological examination typically administered hourly or
bihourly, and their ability to detect early signs of neurological deterioration can make a
difference in further brain injury and survival.33
7.2 DOES NEUROCRITICAL CARE EXPERTISE M AKE A DIFFERENCE?
Several studies have convincingly demonstrated that ICU patients must be treated by
physicians specialised in critical care medicine. A recent meta-analysis of 12 studies
encompassing 24,520 critically ill neurologic patients revealed a clear reduction in
mortality and improved neurologic outcomes for patients cared for in a specialised
critical care unit.34 The subspecialty neurocritical care, which requires additional
training by physicians and nurses, demonstrates its value both to patients and
hospitals. Studies show that it can improve mortality and outcomes and decrease ICU
and hospital length of stay as well as the total cost of care.35
7.3 DOES O RGANISED STROK E UNIT CARE M AKE A D IFFERENCE?
Organised stroke unit care is a form of care provided in hospital by nurses, doctors
and therapists who specialise in treating stroke patients and who work as a
coordinated team. Stroke units, particularly comprehensive stroke units, combine
critical care and rehabilitation.36 The current Stroke-Unit-Trialists’ Collaboration
Cochrane systematic review of 28 trials, involving 5855 participants, showed that
patients who receive this organised stroke unit care are more likely to survive their
stroke, return home and become independent in looking after themselves.37
Stroke Nurse Certificate: Module 19 18
Quality Management
O RG ANISED S TRO K E UNITS IMP RO V E SUR V IV AL A ND THE AB ILITY O F
STR O KE P ATIEN TS TO RE SUM E AN IN DEPE NDE NT LIFE.
The establishment of stroke units should follow the criteria set out in recommendations
of international scientific organisations (e.g. AHA/ASA38, ESO39). The ESO, for example,
has established criteria for stroke unit certification. These criteria are not
recommendations on how to treat stroke patients in stroke units, but they concentrate
on evidence-based recommendations regarding how to structure and organise a
modern stroke unit in a continuum of care.40 The ESO recommendations are focused
on the infrastructural components and processes of stroke units and stroke centres to
make optimal stroke management possible.
Numerous guidelines and recommendations from professional organisations exist.
Most recently, the AHA/ASA guidelines for the early management of patients with
acute ischemic stroke were updated. The guidelines present the current evidence and
management recommendations for evaluation and treatment of adults with acute
ischemic stroke and support an overarching concept of stroke systems of care.41
The implementation of the ESO and AHA/ASA recommendations implicate a multi-
professional team approach, which means that stroke units must be staffed with
physicians, nurses, physiotherapists, occupational therapists, speech and swallowing
therapists, neuropsychologists and a case manager with special interest, training, and
expertise in stroke care. This requires training of the stroke nurses who will be part of
interdisciplinary stroke teams and who will play an important role in the clinical
assessment and treatment of patients with an acute stroke, including cases of stroke
caused by bleeding or sinus venous thrombosis.
In a case study approach, Burton et al. highlighted in a recent study the importance of
an overarching stroke model to guide the organisation of care and the development of
specialist and advanced nursing roles.42 Among the opportunities for role and practice
development, multidisciplinary working, a coordinated approach to education and
training, clinical leadership and a commitment to research appear to be key
organisational features of stroke unit nursing.
Although a case-study approach, the results of the study from Burton et al. are
consistent with findings in the field of evidence-based dissemination and
implementation research in healthcare. In this field of research, it could be shown that
the development and implementation of guidelines alone are usually insufficient to
improve the quality of healthcare.43 Also, many methods can be used to support the
translation of evidence into practice, especially educational interventions are able to
support the knowledge translation.44
Stroke Nurse Certificate: Module 19 19
Quality Management
8 LEADERSHIP AND MANAGEMENT IMPLICATIONS 45
Associated with the paradigm shift from quality assurance to Total Quality
Management came the expectation that accredited organisations become skilled at the
art and science of continuous quality improvement. This included the concepts of
leadership involvement, a commitment to customers’ needs (i.e. patients and families),
an understanding of the principle of process versus people, a devotion to data
collection and analysis as the foundation for problem solving and the view that
multidisciplinary teams working within the processes were the experts and, therefore,
best equipped to drive change and improvement.
KE Y O RG ANISAT IO NA L FEAT URE OF STR O KE NUR SIN G:
M ULTIDISC IP LIN AR Y WO R KING, CO O R DIN ATE D APP RO AC H TO EDUC ATIO N
AN D TRA IN IN G, CLINICAL LE ADE RSHIP A ND CO M MITM EN T TO RE SEA RC H.
Nurse managers in certified organisations were expected to learn these principles and
tools for quality improvement (see above), educate staff in these tools and techniques,
identify improvement opportunities on their units and to be able to be able to interpret
and comment on process changes that occurs a result of data analysis.
They must also be able to participate in organisation-wide improvement teams,
designed to address overarching problem resolution or process redesign projects.
Nurse managers should receive training in facilitation and group meeting techniques, in
addition to the quality improvement techniques. This will enable them to promote a
team-based model of cross-functional problem solving that becomes the standard for
most organisations. Skills and expertise in the concepts of team building, conflict
resolution, statistical process control, customer service and process improvement
continue to be needed by nurse leaders in the future.
Leadership roles and management functions inherent in continuous quality
improvement are delineated in Table 5.46
TABLE 5: LEADERSHIP ROLES AND MANAGEMENT FUNCTIONS
ASSOCIATED W ITH QUALITY IMPROVEMENT
LEADERSHIP ROLES
1 Encourages followers to be actively involved in the quality control process.
2 Clearly communicates expected standards of care to subordinates.
3 Embraces and champions quality improvement as an ongoing process.
Act as a role model for followers in accepting responsibility and accountability for
4
nursing actions.
Supports or actively participates in research efforts to identify and measure nursing
5
sensitive patient outcomes.
MANAGEMENT FUNCTIONS
In conjunction with other personnel in the organisation, establishes clear- cut,
1 measurable standards of care and determines the most appropriate method for
measuring if those standards have been met.
Selects and uses structure, process and outcome audits appropriately as quality
2
control tools.
Stroke Nurse Certificate: Module 19 20
Quality Management
Determines discrepancies between care provided and evidence-based standards and
3
seeks further information regarding why standards were not met.
Keeps abreast of current government, accrediting body, and licensing regulations that
4
affect quality management.
Actively participates in state and national benchmarking and “best practices”
5
initiatives.
Stroke Nurse Certificate: Module 19 21
Quality Management
9 TEST YOURSELF
QUESTION 1: Explain the concept of “Total Quality Management”.
Include in your answer the four core principles of TQM
QUESTION 2: There is extensive literature on the effectiveness of various strategies
to continuously improve quality and performance in the healthcare
organisation.
What strategies would you propose to improve quality in a stroke unit?
Describe at least four different strategies.
Stroke Nurse Certificate: Module 19 22
Quality Management
QUESTION 3: To improve the quality of care, quality must be measured.
Provide an overview of six possible quality measures and their
definitions for a stroke unit.
In your overview, you should distinguish between structural measures,
process measures and outcome measures.
QUESTION 4: Explain the concept of “benchmarking” using a concrete example.
Stroke Nurse Certificate: Module 19 23
Quality Management
QUESTION 5: What is the difference between an organisational standard of care
and an evidence-based guideline?
QUESTION 6: The implementation of a critical incident reporting system (CIRS) is
a key element of risk management.
Explain the CIRS approach, including, in particular, the special focus
and the ultimate goal of the system.
Stroke Nurse Certificate: Module 19 24
Quality Management
QUESTION 7: An organised stroke unit care will improve survival and the ability of
stroke patients to resume an independent life.
What is meant by an “organised stroke unit care”?
Include in your answer a brief explanation of the ESO and AHA/ASA
recommendations
Stroke Nurse Certificate: Module 19 25
Quality Management
10 LITERATURE
Burns, J.D.; Green, D.M.; Metivier, K.; DeFusco, C. (2012): Intensive care management of
acute ischemic stroke. In: Emergency Medicine Clinics of North America; 30, p. 713–744.
Burton, C.R.; Fisher, A.; Green, T.L. (2009): The organisational context of nursing care in
stroke units: A case study approach. In: International Journal of Nursing Studies; 146: p.
86–95.
Chang, C. W. J. (2013): Neurointensive Care Medicine as an Emerging ICU Sub-
specialty. In: Layon, A. J.; Gabrielli, A.; Friedman, W. A. (Ed.): Textbook of
Neurointensive Care. Springer, London, p. 19–30.
Dale, C.; Curtis, J. R. (2014): Quality Improvement in the Intensive Care Unit. In: Scales,
D. C.; Rubenfeld, G. D. (Ed.) (2014): The Organisation of Critical Care. An Evidence
Based Approach to Improving Quality. Springer, New York.
Donabedian, A. (1966): Evaluating the Quality of Medical Care. In: The Milbank Memorial
fund quarterly, 44, 3, p. 166–203.
Grimshaw, J.; Freemantle, N., Wallace, S. et al. (1995): Developing and implementing
clinical practice guidelines. In: Quality in Health Care; 4: p. 55–64.
Haynes AB et al. (2009): A surgical safety checklist to reduce morbidity and mortality
in a global population. N Engl J Med. 2009 Jan 29; 360(5):491-499.
Hollingsworth, N. (2008): Benchmarking. In: Feldman, H. R. (Ed.): Nursing leadership: a
concise encyclopaedia. Springer Publishing, New York, p. 69–71.
Huber, D. L. (2010): Leadership and Nursing Care Management. Sunders
Elsevier, St. Louis.
Hutchinson, A.; Estabrooks, C.A. (2009): Educational theories. In: Straus, S.; Tetroe, J.;
Graham, I. D.: Knowledge Translation in Health Care: Moving from Evidence to Practice.
Wiley-Blackwell, Oxford, p. 206–214.
Jauch EC, Saver JL, Adams HP, et al. (2013): Guidelines for the Early
Management of Patients with Acute Ischemic Stroke: A Guideline for Healthcare
Professionals from the American Heart Association/American Stroke Association.
Stroke; 44:870–947.
John, S.; Bleck, T. P. (2013): Neurocritical Care Organisation. In: Layon, A. J.; Gabrielli, A.;
Friedman, W. A. (Ed.): Textbook of Neurointensive Care. Springer, London, p. 3–8.
Komashie, A.; Mousavi, A. (2007): Quality Management in healthcare and industry. A
comparative review and emerging themes. In: Journal of Management History; 13, 4, p.
359 – 370.
Kramer, A. H.; Zygun, D. A. (2011): do Neurocritical Care units save lives?
Measuring the impact of specialised ICU’s. In: Neurocritical Care; 14. P. 329–333.
Lawson, M.; Enneking, F. K.; Mocco, J. D. (2013): Quality Improvement and
Neurocritical Care. In: Layon, A. J.; Gabrielli, A.; Friedman, W. A. (Ed.): Textbook of
Neurointensive Care. Springer, London, p. 9–17.
Stroke Nurse Certificate: Module 19 26
Quality Management
Marquis, B. L. (2009): Leadership roles and management functions in nursing: theory
and application. Wolters Kluwer Health / Lippincott Williams & Wilkins, Philadelphia.
Moeller J, Breinlinger-O'Reilly J, Elser J. (2000): Quality management in German health
care--the EFQM Excellence Model. Int J Health Care Quality Assurance Inc. Leadership
Health Serv. 2000; 13(6-7):254-8.
Norrving B et al. (2015): Cross-National Key Performance Measures of the Quality of
Acute Stroke Care in Western Europe. Stroke. 2015 Oct; 46(10):2891-2895.
Pelletier, L. R.; Albright; l, A. (2010): Quality Improvement and Healthcare Safety.
In: Huber 2010, Leadership and Nursing Care Management, S. 523 f.
Pronovost, A.; Rubenfeld, G. D. (2009): Quality in critical care. In: Chiche, J.-D.; Moreno,
R.; Putensen, C.; Rhodes, A. (Ed.): Patient Safety and Quality of care in Intensive Care
Medicine. Medizinisch wissenschaftliche Verlagsgesellschaft, Berlin, p. 127–139.
Ringelstein, E. B.; Chamorro, A.; Kaste, M. et al. (2013): European Stroke
Organisation Recommendations to Establish a Stroke Unit and Stroke Centre. In:
Stroke; 44, p. 828–840.
Sánchez E et al. (2006): A descriptive study of the implementation of the EFQM
excellence model and underlying tools in the Basque Health Service. Int J Qual Health
Care. 2006 Feb; 18(1):58-65.
Sauser K et al. (2014): A systematic review and critical appraisal of quality measures for
the emergency care of acute ischemic stroke. Ann Emerg Med. 2014 Sep; 64(3):235-
244.
Stroke-Unit-Trialists’-Collaboration (2013): Organised inpatient (stroke unit) care for
stroke. In: Cochrane Database of Systematic Reviews. Art. No.: CD000197.
(http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD000197.pub3/abstract)
Sullivan, E. J.; Decker, P. J. (2009): Effective Leadership and Management in Nursing.
Pearson Education, London.
Wiedmann S, et al. on behalf of the German Stroke Registers Study Group (ADSR)
(2014): The quality of acute stroke care- an analysis of evidence- based indicators in
260 000 patients. Dtsch Arztebl Int. 2014 Nov 7; 111(45):759-65.
Wojner-Alexandrov, A. W. (2008): Outcomes Management. In: Feldman, H. R. (Ed.):
Nursing leadership: a concise encyclopaedia. Springer Publishing, New York, p. 434–
438.
Stroke Nurse Certificate: Module 19 27
Quality Management
11 APPENDIX
19 EVIDENCE-BASED QUALITY INDICATORS OF THE GERMAN STROKE REGISTRY TO
MONITOR THE QUALITY OF STROKE CARE IN GERMAN STROKE UNITS (WIEDMANN
ET AL. 2014)
11.1 DEFINITION O F Q UALITY INDICATORS
1. Antithrombotic therapy - antiaggregation ≤ 48h after stroke
Numerator: Number of patients receiving platelet inhibitors within the first 48 hours
after the stroke.
Denominator: All patients with TIA or cerebral infarction. Excluded are: patients
receiving anticoagulation, patients <18 years, and patients with interval onset to
admission >48 h.
Reference/target range: ≥95%
2. Antithrombotic therapy - antiaggregation as secondary prophylaxis
Numerator: Number of patients receiving platelet inhibitors at discharge
Denominator: All patients with TIA or cerebral infarction. Patients receiving
anti-coagulation, patients <18 years, and patients with discharge status “deceased” are
excluded.
Reference/target range: ≥95%
3. Antithrombotic therapy - anticoagulation in atrial fibrillation
Numerator: Number of patients receiving therapeutic anticoagulation at discharge or
with a recommendation for anticoagulation in their discharge notes
Denominator: All patients with TIA or cerebral infarction and atrial fibrillation, who are
discharged home or to a rehabilitation hospital and are mobile (operationalised by
using categories 10–15 in item “change of position from bed to chair” and categories
10–15 in item “locomotion” in the Barthel index at dis- charge) and minimally impaired
(operationalised by using Rankin scale 0–3 at discharge); patients <18 are excluded.
Reference/target range: ≥80%
4. Brain imaging in patients with suspected stroke
Numerator: Number of patients receiving brain imaging (CCT and/or NMR)
Denominator: All documented patients
Reference/target range: ≥95%
5. Vascular imaging in cerebral infarction and TIA
Numerator: All patients with extracranial vascular imaging (Doppler ultrasound and/or
duplex sonography and/or digital subtraction angiography and/or magnetic
resonance/computed tomography angiography)
Denominator: All patients with cerebral infarction or TIA
Reference/target range: ≥90%
Stroke Nurse Certificate: Module 19 28
Quality Management
6. Screening for dysphagia
Numerator: All patients with swallowing test according to protocol with minimal
requirements (for example, “includes stepwise water swallowing test of at least
50/mL”)
Denominator: All patients with stroke and a minimum stay ≥ 1 day; patients with TIA
and patients with impaired consciousness are excluded
Reference/target range: ≥90%
7. Early rehabilitation—physiotherapy/occupational therapy
Numerator: Number of patients examined by and/or receiving treatment from a
physiotherapist and/or occupational therapist ≤ day 2 after admission
Denominator: All patients with documented paresis and notable functional
impairment (Rankin scale ≥ 3 and/or sum Barthel index ≤ 70 within the first 24 hours
after admission) with a minimum stay of ≥ 1 day; patients who are comatose at the time
of admission and patients with a diagnosis of TIA are excluded
Reference/target range: ≥90%
8. Early rehabilitation—speech therapy
Numerator: Number of patients who were examined by and/or received treatment
from a speech therapist ≤ day 2 after admission
Denominator: All patients with documented aphasia and/or dysarthria and/or
dysphagia at admission and a minimum stay of ≥ 1 day. Patients who are comatose at
the time of admission and patients with TIA are excluded
Reference/target range: ≥80%
9. Early mobilisation
Numerator: Number of patients who were mobilised within 2 days after admission
Denominator: All patients who changed position from bed to chair “with support” or
found it “impossible” (operationalised by categories 0–10 in item “change of position
from bed to chair” in the Barthel index within the first 24 hours after admission) with a
minimum stay ≥ 1 day; patients with TIA and/or intracranial pressure and/or ventilation
and/or coma at admission are excluded
Reference/target range: ≥90%
10. Information for patients and their relatives
Numerator: Number of patients (or their relatives) who received verbal and written
information before discharge
• On the disease course/prevention by the doctor
• On support offers by social/care services
Denominator: Patients with a minimum length of stay ≥ 1 day; patients with a
diagnosis of TIA and patients with a discharge status “deceased” were excluded
Reference/target range: ≥90%
Stroke Nurse Certificate: Module 19 29
Quality Management
11. Patients with brain imaging within 1 h of admission in patients admitted
within 2h after stroke onset
Numerator: All patients with interval admission to first imaging procedure (CCT
and/or MRI) ≤ 1 h
Denominator: All patients with interval between onset and admission ≤ 2 h and
sufficient stroke severity to receive intravenous thrombolysis (NIHSS 4–25) and age
between 18 and 80 years
Reference/target range: ≥90%
12. Early systemic thrombolytic therapy in eligible patients
Numerator: All patients receiving intravenous thrombolysis
Denominator: All patients with cerebral infarction and a time interval between onset
and admission of ≥ 2 hours, as well as sufficient stroke severity to conduct intravenous
thrombolysis (NIHSS 4–25), aged between 18 and 80 years. Patients with intra-arterial
thrombolysis are excluded.
Reference/target range: ≥60%
13. Pneumonia rate after stroke
Numerator: Number of patients with pneumonia as a complication
Denominator: All patients with cerebral infarction
Reference/target range: —
14. In-hospital mortality after acute stroke
Numerator: Number of patients with discharge status deceased on day 7
Denominator: All patients with cerebral infarction. Patients with length of stay ≤ 7
days and who were discharged into another acute hospital, other department,
rehabilitation ward, or care home are excluded
Reference/target range: —
15. Mortality after thrombolysis (since 2010)
Numerator: Patients who died within 7 days after thrombolysis
Denominator: All patients receiving thrombolysis
Reference/target range: —
16. Revascularisation of carotid artery stenosis (since 2010)
Numerator: Patients with a recommendation for revascularisation in their referral
letter, or referral to revascularisation, or who have undergone revascularisation
Denominator: All patients with cerebral infarction/TIA and symptomatic carotid
artery stenosis ≥ 70%
Reference/target range: —
Stroke Nurse Certificate: Module 19 30
Quality Management
17. Door to needle time ≤ 60 min if time between onset and admission ≤ 2 h
(since 2010)
Numerator: Patients with a time window from admission to start of thrombolysis
≤ 60 minutes
Denominator: All patients receiving thrombolysis
Reference/target range: —
18. Treatment in stroke unit (since 2010)
Numerator: Patients admitted to stroke unit
Denominator: All patients with stroke/TIA who were admitted to the hospital
Reference/target range: —
19. Discharge destination rehabilitation of patients w ith impairments
affecting
everyday life (since 2010)
Numerator: All patients with the discharge destination of outpatient or inpatient
rehabilitation (to start imminently, organised and registered by the hospital, not
necessarily direct transfer to rehabilitation)
Denominator: All patient with stroke, mRS 2–5 at discharge, without prior stay in a
care home, age <80. Patients transferred to another acute hospital or ward are
excluded
Reference/target range: —
Stroke Nurse Certificate: Module 19 31
Quality Management
12 REFERENCES
1
Chapter based on Komashie and Mousavi 2007; Donabedian 1966; Huber 2010
2
Donabedian 1966, p. 167
3
Donabedian 1966
4
Table modified according to Komashie and Mousavi 2007, p. 363.
5
Chapter based on Huber 2010, p. 529 f.
6
Chapter based on Sullivan and Decker 2009, p. 79 f.
7
Pelletier/Albright 2010, Sàncez 2006; Moeller et al. 2000.
8
Chapter based on Sullivan and Decker 2009, p. 79 f.
9
Lawson et al. 2013, p. 14 f.
10
Modified according to Pronovost and Rubenfeld 2009, p. 132; Dale/Curtis 2014
11
A bundle is a selected set of elements of care distilled from evidence-based practice
guidelines that, when implemented as a group, have an effect on outcomes beyond
implementing the individual elements alone. For example:
http://www.survivingsepsis.org/Bundles/Pages/default.aspx
12
Haynes et al. 2009
13
Weiss et al. 2011
15
Chapter based on Sullivan and Decker 2009, p. 79 f.; Marquis 2009
16
Marquis 2009, p. 543
17
AHA/ASA = American Heart Association/American Stroke Association
18
ESO = European Stroke Organisation
19
Modified according to John and Bleck 2013, p. 6–7.
20
SU = Stroke Unit
21
NCU = Neurocritical Care Unit
22
EQ-5D™: a system that describes the health-related quality of life states by means of five
dimensions (mobility, self-care, usual activities, pain/discomfort, anxiety/depression). See:
http://www.euroqol.org/home.html
23
Norrving et al. 2015; Sauser et al. 2014
24
Wiedmann et al. 2014
25
Chapter based on Huber 2010, p. 561 f.; Wojner-Alexandrov 2008
26
Donabedian 1966, p. 168
27
Sullivan 2009, p. 79 – only 1.5.4
28
Chapter based on Marquis 2009, p. 540; Hollingsworth 2008
29
Chapter based on Sullivan and Decker 2009, p. 84 f.
30
John and Bleck 2013, p. 3.
31
Chang 2013, p. 20.
32
John and Bleck 2013, p. 4; Chang 2013, p. 23 f.
33
Chang 2013, p. 23.
34
Kramer and Zygun 2011
Stroke Nurse Certificate: Module 19 32
Quality Management
35
Chang 2013, p. 24 f.; Knopf et al. 2012
36
Burns et al. 2012
37
Stroke Unit Trialists’ Collaboration 2013
38
AHA/ASA = American Heart Association/American Stroke Association
39
ESO = European Stroke Organisation
40
Ringelstein et al. 2013
41
Jauch et al. 2013
42
Burton et al. 2009
43
Grimshaw et al. 1995
44
Hutchinson et al. 2009
45
Huber 2010, p. 540 f.
46
Marquis et al. 2009, p. 539
Stroke Nurse Certificate: Module 19 33
Quality Management
You might also like
- APTA Clinical Practice Guideline Process ManualNo ratings yetAPTA Clinical Practice Guideline Process Manual63 pages
- Quality Assurance in Nursing Main ContentNo ratings yetQuality Assurance in Nursing Main Content32 pages
- Quality in Healthcare Organization: Fariday 1No ratings yetQuality in Healthcare Organization: Fariday 137 pages
- Quality Management in Health Care: Concepts, Principles and StandardsNo ratings yetQuality Management in Health Care: Concepts, Principles and Standards8 pages
- Quality Management in Health Care: Concepts, Principles and StandardsNo ratings yetQuality Management in Health Care: Concepts, Principles and Standards8 pages
- IJPRABriefreviewon Total Quality Managementin Pharmaceutical IndustriesNo ratings yetIJPRABriefreviewon Total Quality Managementin Pharmaceutical Industries10 pages
- كتاب اساسيات الجودة والامان فى التمريض قسم ادارة التمريضNo ratings yetكتاب اساسيات الجودة والامان فى التمريض قسم ادارة التمريض58 pages
- Perkembangan Serta Program Menjaga Mutu Pelayanan KesehatanNo ratings yetPerkembangan Serta Program Menjaga Mutu Pelayanan Kesehatan44 pages
- NapulanRM - CQI in Records and Clinical Documentation ImprovementNo ratings yetNapulanRM - CQI in Records and Clinical Documentation Improvement92 pages
- Quality Indicator - A Tool For Quality Monitoring and ImprovingNo ratings yetQuality Indicator - A Tool For Quality Monitoring and Improving5 pages
- Quality Management System (QMS) Http://iaetsdjaras - OrgNo ratings yetQuality Management System (QMS) Http://iaetsdjaras - Org7 pages
- 20230815_Total Quality Management for Trauma_Malaysia Society for the Care of Trauma_MASCOTNo ratings yet20230815_Total Quality Management for Trauma_Malaysia Society for the Care of Trauma_MASCOT64 pages
- Process Validation of Paracetamol Tablets A CompreNo ratings yetProcess Validation of Paracetamol Tablets A Compre10 pages
- Day 12 Implementing Quality Improvement ProgramNo ratings yetDay 12 Implementing Quality Improvement Program23 pages
- Guide For Clinical Audit Leads 21 Mar 11No ratings yetGuide For Clinical Audit Leads 21 Mar 1140 pages
- A Book Review: Master of Arts in NursingNo ratings yetA Book Review: Master of Arts in Nursing20 pages
- John Davies - Quality, Evidence and Effectiveness in Health Promotion_ Striving for Certainties (1998)No ratings yetJohn Davies - Quality, Evidence and Effectiveness in Health Promotion_ Striving for Certainties (1998)238 pages
- Quality Assurance & Certification Syllabus, IntroductionNo ratings yetQuality Assurance & Certification Syllabus, Introduction27 pages
- Total Quality Management in Healthcare TNo ratings yetTotal Quality Management in Healthcare T5 pages
- Managing Quality vs. Measuring Uncertainty in The Medical LaboratoryNo ratings yetManaging Quality vs. Measuring Uncertainty in The Medical Laboratory11 pages
- Using ISO 9001 in Healthcare: Applications for Quality Systems, Performance Improvement, Clinical Integration, Accreditation, and Patient SafetyFrom EverandUsing ISO 9001 in Healthcare: Applications for Quality Systems, Performance Improvement, Clinical Integration, Accreditation, and Patient SafetyNo ratings yet
- JCI Accreditation Standards For Hospitals and Academic Medical Centers (AMC), 8 EditionNo ratings yetJCI Accreditation Standards For Hospitals and Academic Medical Centers (AMC), 8 Edition39 pages
- Risk Assessment and Prevention of Pressure Ulcers100% (2)Risk Assessment and Prevention of Pressure Ulcers131 pages
- CPG Managment of Neonatal Jaundice (Second Edition) NewNo ratings yetCPG Managment of Neonatal Jaundice (Second Edition) New62 pages
- 2016 Toronto ERAS - STOMA - BPS - FINAL - 2018No ratings yet2016 Toronto ERAS - STOMA - BPS - FINAL - 201825 pages
- Collection, Transport and Storage of Specimens For Laboratory Diagnosis PDF100% (1)Collection, Transport and Storage of Specimens For Laboratory Diagnosis PDF25 pages
- CPG Management of Haemophilia 20191024 PDFNo ratings yetCPG Management of Haemophilia 20191024 PDF21 pages
- ccpc15 Practice Administration and Development Protocol Development Workbook100% (1)ccpc15 Practice Administration and Development Protocol Development Workbook26 pages
- Darren L. Mungcal BSN 123 Group 92 Evidence Based NursingNo ratings yetDarren L. Mungcal BSN 123 Group 92 Evidence Based Nursing6 pages
- Impact of Overall Quality Management and Its Impact On Care HomesNo ratings yetImpact of Overall Quality Management and Its Impact On Care Homes18 pages
- Anaphylaxis in Children and Adults Prevention, Diagnosis and Treatment100% (1)Anaphylaxis in Children and Adults Prevention, Diagnosis and Treatment88 pages
- Worldviews Ev Based Nurs - 2022 - Schoberer - Fall Prevention in Hospitals and Nursing Homes Clinical Practice GuidelineNo ratings yetWorldviews Ev Based Nurs - 2022 - Schoberer - Fall Prevention in Hospitals and Nursing Homes Clinical Practice Guideline8 pages
- Omnibus Health Guidelines For Adults Version 2023100% (1)Omnibus Health Guidelines For Adults Version 2023216 pages
- ADA Guideline - Chronic Kidney Disease Evidence-Based Nutrition Practice GuidelineNo ratings yetADA Guideline - Chronic Kidney Disease Evidence-Based Nutrition Practice Guideline19 pages

























































































- Quality Management in Health Care: Concepts, Principles and StandardsQuality Management in Health Care: Concepts, Principles and Standards
- Quality Management in Health Care: Concepts, Principles and StandardsQuality Management in Health Care: Concepts, Principles and Standards
- IJPRABriefreviewon Total Quality Managementin Pharmaceutical IndustriesIJPRABriefreviewon Total Quality Managementin Pharmaceutical Industries
- كتاب اساسيات الجودة والامان فى التمريض قسم ادارة التمريضكتاب اساسيات الجودة والامان فى التمريض قسم ادارة التمريض
- Perkembangan Serta Program Menjaga Mutu Pelayanan KesehatanPerkembangan Serta Program Menjaga Mutu Pelayanan Kesehatan
- NapulanRM - CQI in Records and Clinical Documentation ImprovementNapulanRM - CQI in Records and Clinical Documentation Improvement
- Quality Indicator - A Tool For Quality Monitoring and ImprovingQuality Indicator - A Tool For Quality Monitoring and Improving
- Quality Management System (QMS) Http://iaetsdjaras - OrgQuality Management System (QMS) Http://iaetsdjaras - Org
- 20230815_Total Quality Management for Trauma_Malaysia Society for the Care of Trauma_MASCOT20230815_Total Quality Management for Trauma_Malaysia Society for the Care of Trauma_MASCOT
- Process Validation of Paracetamol Tablets A CompreProcess Validation of Paracetamol Tablets A Compre
- John Davies - Quality, Evidence and Effectiveness in Health Promotion_ Striving for Certainties (1998)John Davies - Quality, Evidence and Effectiveness in Health Promotion_ Striving for Certainties (1998)
- Quality Assurance & Certification Syllabus, IntroductionQuality Assurance & Certification Syllabus, Introduction
- Managing Quality vs. Measuring Uncertainty in The Medical LaboratoryManaging Quality vs. Measuring Uncertainty in The Medical Laboratory
- Using ISO 9001 in Healthcare: Applications for Quality Systems, Performance Improvement, Clinical Integration, Accreditation, and Patient SafetyFrom EverandUsing ISO 9001 in Healthcare: Applications for Quality Systems, Performance Improvement, Clinical Integration, Accreditation, and Patient Safety
- JCI Accreditation Standards For Hospitals and Academic Medical Centers (AMC), 8 EditionJCI Accreditation Standards For Hospitals and Academic Medical Centers (AMC), 8 Edition
- CPG Managment of Neonatal Jaundice (Second Edition) NewCPG Managment of Neonatal Jaundice (Second Edition) New
- Collection, Transport and Storage of Specimens For Laboratory Diagnosis PDFCollection, Transport and Storage of Specimens For Laboratory Diagnosis PDF
- ccpc15 Practice Administration and Development Protocol Development Workbookccpc15 Practice Administration and Development Protocol Development Workbook
- Darren L. Mungcal BSN 123 Group 92 Evidence Based NursingDarren L. Mungcal BSN 123 Group 92 Evidence Based Nursing
- Impact of Overall Quality Management and Its Impact On Care HomesImpact of Overall Quality Management and Its Impact On Care Homes
- Anaphylaxis in Children and Adults Prevention, Diagnosis and TreatmentAnaphylaxis in Children and Adults Prevention, Diagnosis and Treatment
- Worldviews Ev Based Nurs - 2022 - Schoberer - Fall Prevention in Hospitals and Nursing Homes Clinical Practice GuidelineWorldviews Ev Based Nurs - 2022 - Schoberer - Fall Prevention in Hospitals and Nursing Homes Clinical Practice Guideline
- ADA Guideline - Chronic Kidney Disease Evidence-Based Nutrition Practice GuidelineADA Guideline - Chronic Kidney Disease Evidence-Based Nutrition Practice Guideline