The nursing care plan is for a patient with chronic renal failure secondary to diabetes nephropathy. The nursing diagnosis is a risk for ineffective protection related to an abnormal blood profile. Nursing interventions include hand washing, limiting visitors to prevent infection transmission, monitoring for signs of fatigue and infection, and changing the ventriculostomy dressing regularly. After 7-8 hours the patient's condition was stable with no increased intracranial pressure, further deterioration, and stable vital signs.
Copyright:
Attribution Non-Commercial (BY-NC)
Available Formats
Download as DOC, PDF, TXT or read online from Scribd
The nursing care plan is for a patient with chronic renal failure secondary to diabetes nephropathy. The nursing diagnosis is a risk for ineffective protection related to an abnormal blood profile. Nursing interventions include hand washing, limiting visitors to prevent infection transmission, monitoring for signs of fatigue and infection, and changing the ventriculostomy dressing regularly. After 7-8 hours the patient's condition was stable with no increased intracranial pressure, further deterioration, and stable vital signs.
The nursing care plan is for a patient with chronic renal failure secondary to diabetes nephropathy. The nursing diagnosis is a risk for ineffective protection related to an abnormal blood profile. Nursing interventions include hand washing, limiting visitors to prevent infection transmission, monitoring for signs of fatigue and infection, and changing the ventriculostomy dressing regularly. After 7-8 hours the patient's condition was stable with no increased intracranial pressure, further deterioration, and stable vital signs.
Copyright:
Attribution Non-Commercial (BY-NC)
Available Formats
Download as DOC, PDF, TXT or read online from Scribd
The nursing care plan is for a patient with chronic renal failure secondary to diabetes nephropathy. The nursing diagnosis is a risk for ineffective protection related to an abnormal blood profile. Nursing interventions include hand washing, limiting visitors to prevent infection transmission, monitoring for signs of fatigue and infection, and changing the ventriculostomy dressing regularly. After 7-8 hours the patient's condition was stable with no increased intracranial pressure, further deterioration, and stable vital signs.
Copyright:
Attribution Non-Commercial (BY-NC)
Available Formats
Download as DOC, PDF, TXT or read online from Scribd
Download as doc, pdf, or txt
You are on page 1/ 5
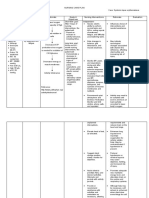
NURSING CARE PLAN
Name of Patient: X Medical Diagnosis: Chronic renal failure secondary to DM nephropathy.
Nursing Diagnosis: Risk for ineffective protection related to abnormal blood profile.
Findings Expected Outcome Nursing Interventions and Rationale Actual Evaluation
O= Received patient on bed, Within 8 hours of nursing -Hand washing and observe proper medical asepsis and limit visitors. After 7-8 hours of nursing awake, conscious with intervention, the patient will R= to limit transmission of infections since the patient has a weak intervention, the patient was: intravenous fluid of # 1 D5 be able to: immune system. 0.3% NaCl 500cc @ KVO, 1. Still in coma, no signs of infusing well at left arm. 1. Experience no signs/ -Note reports of increasing fatigue, weakness. Observe for tachycardia, increased ICP noted. > With ventriculostomy tube symptoms of bleeding. pallor of skin/ mucous membranes, dyspnea , and chest pain. Plan patient freely draining to blood bag; activities to avoid fatigue. 2. Displayed no further dressing is dry and intact. 2. Maintain / demonstrate R=May reflect effects of anemia and cardiac response. To let the patient deterioration. > With traeostomy attached improvement in laboratory rest. to mechanical ventilator, values. 3. With stable vital signs of with FIO2 of 80%. -Note for the sign of infections in the operative site and change the >T=36.8oC. > With nasogastric tube for dressing regularly. >P= 101 bpm. feeding. R= since the patient undergone ventriculostomy, noting and changing the >R= 21 cpm. WBC= 20T dressing can help minimize the infection. >BP=140/80mmhg RBC= 3.5 million/uL > With the following vital signs of: >T=36.5oC. >P=100bpm. >R= 22 cpm. >BP=130/80mmhg
Noted By:
Senior/ Staff Nurse & Nurse Supervisor
NURSING CARE PLAN
Name of Patient: X Medical Diagnosis: Acute Myocardial Infarction
Nursing Diagnosis: Infective Tissue Perfusion related to Poor Myocardial Contractility
Findings Expected Outcome Nursing Interventions and Rationale Actual Evaluation
O= Received patient on bed, Within 8 hours of nursing -Hand washing and observe proper medical asepsis and limit visitors. After 7-8 hours of nursing awake, conscious with intervention, the patient will R= to limit transmission of infections since the patient has a weak intervention, the patient was: intravenous fluid of # 1 D5 be able to: immune system. 0.3% NaCl 500cc @ KVO, 1. Still in coma, no signs of infusing well at left arm. 1. Experience no signs/ -Note reports of increasing fatigue, weakness. Observe for tachycardia, increased ICP noted. > With ventriculostomy tube symptoms of bleeding. pallor of skin/ mucous membranes, dyspnea , and chest pain. Plan patient freely draining to blood bag; activities to avoid fatigue. 2. Displayed no further dressing is dry and intact. 2. Maintain / demonstrate R=May reflect effects of anemia and cardiac response. To let the patient deterioration. > With traeostomy attached improvement in laboratory rest. to mechanical ventilator, values. 3. With stable vital signs of with FIO2 of 80%. -Note for the sign of infections in the operative site and change the >T=36.8oC. > With nasogastric tube for dressing regularly. >P= 101 bpm. feeding. R= since the patient undergone ventriculostomy, noting and changing the >R= 21 cpm. WBC= 20T dressing can help minimize the infection. >BP=140/80mmhg RBC= 3.5 million/uL > With the following vital signs of: >T=36.5oC. >P=100bpm. >R= 22 cpm. >BP=130/80mmhg
Noted By:
Senior/ Staff Nurse & Nurse Supervisor
NURSING CARE PLAN
Name of Patient: X Medical Diagnosis:
Nursing Diagnosis: Infective Tissue Perfusion related to Poor Myocardial Contractility
Findings Expected Outcome Nursing Interventions and Rationale Actual Evaluation
O= Received patient on bed, Within 8 hours of nursing -Hand washing and observe proper medical asepsis and limit visitors. After 7-8 hours of nursing awake, conscious with intervention, the patient will R= to limit transmission of infections since the patient has a weak intervention, the patient was: intravenous fluid of # 1 D5 be able to: immune system. 0.3% NaCl 500cc @ KVO, 1. Still in coma, no signs of infusing well at left arm. 1. Experience no signs/ -Note reports of increasing fatigue, weakness. Observe for tachycardia, increased ICP noted. > With ventriculostomy tube symptoms of bleeding. pallor of skin/ mucous membranes, dyspnea , and chest pain. Plan patient freely draining to blood bag; activities to avoid fatigue. 2. Displayed no further dressing is dry and intact. 2. Maintain / demonstrate R=May reflect effects of anemia and cardiac response. To let the patient deterioration. > With traeostomy attached improvement in laboratory rest. to mechanical ventilator, values. 3. With stable vital signs of with FIO2 of 80%. -Note for the sign of infections in the operative site and change the >T=36.8oC. > With nasogastric tube for dressing regularly. >P= 101 bpm. feeding. R= since the patient undergone ventriculostomy, noting and changing the >R= 21 cpm. WBC= 20T dressing can help minimize the infection. >BP=140/80mmhg RBC= 3.5 million/uL > With the following vital signs of: >T=36.5oC. >P=100bpm. >R= 22 cpm. >BP=130/80mmhg
Noted By:
Senior/ Staff Nurse & Nurse Supervisor
NURSING CARE PLAN
Name of Patient: X Medical Diagnosis:
Nursing Diagnosis: Infective Tissue Perfusion related to Poor Myocardial Contractility
Findings Expected Outcome Nursing Interventions and Rationale Actual Evaluation
O= Received patient on bed, Within 8 hours of nursing -Hand washing and observe proper medical asepsis and limit visitors. After 7-8 hours of nursing awake, conscious with intervention, the patient will R= to limit transmission of infections since the patient has a weak intervention, the patient was: intravenous fluid of # 1 D5 be able to: immune system. 0.3% NaCl 500cc @ KVO, 1. Still in coma, no signs of infusing well at left arm. 1. Experience no signs/ -Note reports of increasing fatigue, weakness. Observe for tachycardia, increased ICP noted. > With ventriculostomy tube symptoms of bleeding. pallor of skin/ mucous membranes, dyspnea , and chest pain. Plan patient freely draining to blood bag; activities to avoid fatigue. 2. Displayed no further dressing is dry and intact. 2. Maintain / demonstrate R=May reflect effects of anemia and cardiac response. To let the patient deterioration. > With traeostomy attached improvement in laboratory rest. to mechanical ventilator, values. 3. With stable vital signs of with FIO2 of 80%. -Note for the sign of infections in the operative site and change the >T=36.8oC. > With nasogastric tube for dressing regularly. >P= 101 bpm. feeding. R= since the patient undergone ventriculostomy, noting and changing the >R= 21 cpm. WBC= 20T dressing can help minimize the infection. >BP=140/80mmhg RBC= 3.5 million/uL > With the following vital signs of: >T=36.5oC. >P=100bpm. >R= 22 cpm. >BP=130/80mmhg
Noted By:
Senior/ Staff Nurse & Nurse Supervisor
NURSING CARE PLAN
Name of Patient: X Medical Diagnosis:
Nursing Diagnosis: Infective Tissue Perfusion related to Poor Myocardial Contractility
Findings Expected Outcome Nursing Interventions and Rationale Actual Evaluation
O= Received patient on bed, Within 8 hours of nursing -Hand washing and observe proper medical asepsis and limit visitors. After 7-8 hours of nursing awake, conscious with intervention, the patient will R= to limit transmission of infections since the patient has a weak intervention, the patient was: intravenous fluid of # 1 D5 be able to: immune system. 0.3% NaCl 500cc @ KVO, 1. Still in coma, no signs of infusing well at left arm. 1. Experience no signs/ -Note reports of increasing fatigue, weakness. Observe for tachycardia, increased ICP noted. > With ventriculostomy tube symptoms of bleeding. pallor of skin/ mucous membranes, dyspnea , and chest pain. Plan patient freely draining to blood bag; activities to avoid fatigue. 2. Displayed no further dressing is dry and intact. 2. Maintain / demonstrate R=May reflect effects of anemia and cardiac response. To let the patient deterioration. > With traeostomy attached improvement in laboratory rest. to mechanical ventilator, values. 3. With stable vital signs of with FIO2 of 80%. -Note for the sign of infections in the operative site and change the >T=36.8oC. > With nasogastric tube for dressing regularly. >P= 101 bpm. feeding. R= since the patient undergone ventriculostomy, noting and changing the >R= 21 cpm. WBC= 20T dressing can help minimize the infection. >BP=140/80mmhg RBC= 3.5 million/uL > With the following vital signs of: >T=36.5oC. >P=100bpm. >R= 22 cpm. >BP=130/80mmhg