

Clinical and Genetic Characterization of Patients with Bartter and Gitelman Syndrome
- PMID: 35628451
- PMCID: PMC9144947
- DOI: 10.3390/ijms23105641
Clinical and Genetic Characterization of Patients with Bartter and Gitelman Syndrome
Abstract
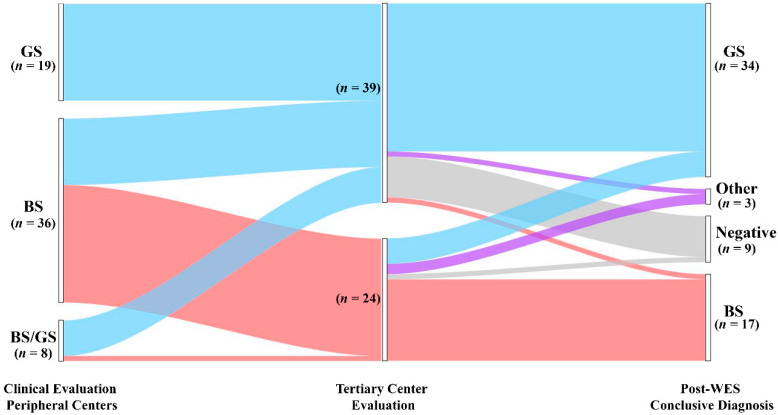
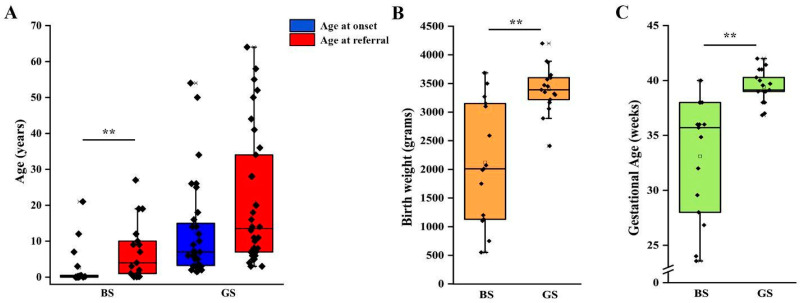
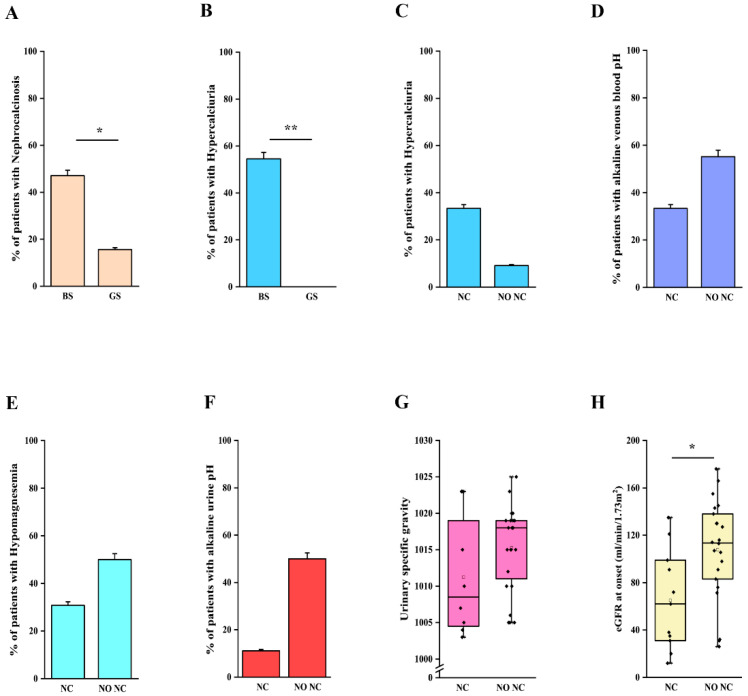
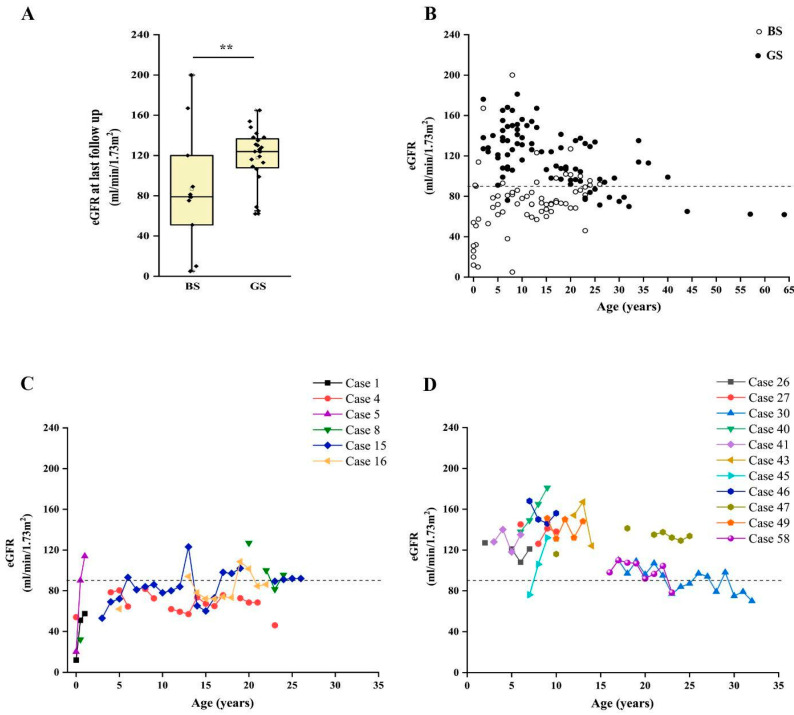
Bartter (BS) and Gitelman (GS) syndrome are autosomal recessive inherited tubulopathies, whose clinical diagnosis can be challenging, due to rarity and phenotypic overlap. Genotype-phenotype correlations have important implications in defining kidney and global outcomes. The aim of our study was to assess the diagnostic rate of whole-exome sequencing (WES) coupled with a bioinformatic analysis of copy number variations in a population of 63 patients with BS and GS from a single institution, and to explore genotype-phenotype correlations. We obtained a diagnostic yield of 86% (54/63 patients), allowing disease reclassification in about 14% of patients. Although some clinical and laboratory features were more commonly reported in patients with BS or GS, a significant overlap does exist, and age at onset, preterm birth, gestational age and nephro-calcinosis are frequently misleading. Finally, chronic kidney disease (CKD) occurs in about 30% of patients with BS or GS, suggesting that the long-term prognosis can be unfavorable. In our cohort the features associated with CKD were lower gestational age at birth and a molecular diagnosis of BS, especially BS type 1. The results of our study demonstrate that WES is useful in dealing with the phenotypic heterogeneity of these disorders, improving differential diagnosis and genotype-phenotype correlation.
Keywords: Bartter syndrome; Gitelman syndrome; chronic kidney disease; genetics; salt-losing tubulopathies; whole-exome sequencing.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Congenital chloride diarrhea needs to be distinguished from Bartter and Gitelman syndrome.J Hum Genet. 2018 Jul;63(8):887-892. doi: 10.1038/s10038-018-0470-7. Epub 2018 May 30. J Hum Genet. 2018. PMID: 29849040
-
Inherited salt-losing tubulopathy: An old condition but a new category of tubulopathy.Pediatr Int. 2020 Apr;62(4):428-437. doi: 10.1111/ped.14089. Epub 2020 Apr 13. Pediatr Int. 2020. PMID: 31830341 Review.
-
Differential diagnosis of Bartter syndrome, Gitelman syndrome, and pseudo-Bartter/Gitelman syndrome based on clinical characteristics.Genet Med. 2016 Feb;18(2):180-8. doi: 10.1038/gim.2015.56. Epub 2015 Apr 16. Genet Med. 2016. PMID: 25880437
-
Bartter syndrome representing digenic-based salt-losing tubulopathies presumably accelerated by renal insufficiency.CEN Case Rep. 2020 Nov;9(4):375-379. doi: 10.1007/s13730-020-00489-3. Epub 2020 Jun 6. CEN Case Rep. 2020. PMID: 32506365 Free PMC article.
-
Bartter and Gitelman syndromes.Cas Lek Cesk. 2022 Summer;161(3-4):131-134. Cas Lek Cesk. 2022. PMID: 36100451 Review. English.
Cited by
-
Clinical, genetic characteristics and outcome of four Chinese patients with Bartter syndrome type 3: Further insight into a genotype-phenotype correlation.Mol Genet Metab Rep. 2024 Jul 5;40:101112. doi: 10.1016/j.ymgmr.2024.101112. eCollection 2024 Sep. Mol Genet Metab Rep. 2024. PMID: 39071140 Free PMC article.
References
-
- Blanchard A., Bockenhauer D., Bolignano D., Calò L.A., Cosyns E., Devuyst O., Ellison D.H., Karet Frankl F.E., Knoers N.V.A.M., Konrad M., et al. Gitelman Syndrome: Consensus and Guidance from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int. 2017;91:24–33. doi: 10.1016/j.kint.2016.09.046. - DOI - PubMed
-
- Bokhari S.R.A., Zulfiqar H., Mansur A. StatPearls. StatPearls Publishing; Treasure Island, FL, USA: 2022. Bartter Syndrome. - PubMed
-
- Konrad M., Nijenhuis T., Ariceta G., Bertholet-Thomas A., Calo L.A., Capasso G., Emma F., Schlingmann K.P., Singh M., Trepiccione F., et al. Diagnosis and Management of Bartter Syndrome: Executive Summary of the Consensus and Recommendations from the European Rare Kidney Disease Reference Network Working Group for Tubular Disorders. Kidney Int. 2021;99:324–335. doi: 10.1016/j.kint.2020.10.035. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
