

Muscle and Bone Impairment in Infantile Nephropathic Cystinosis: New Concepts
- PMID: 35011732
- PMCID: PMC8749987
- DOI: 10.3390/cells11010170
Muscle and Bone Impairment in Infantile Nephropathic Cystinosis: New Concepts
Abstract
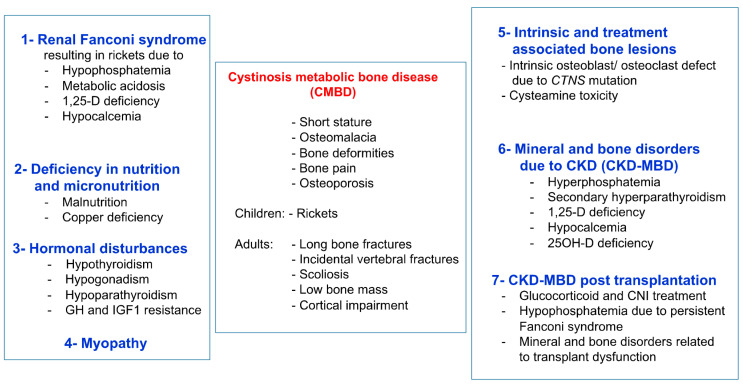
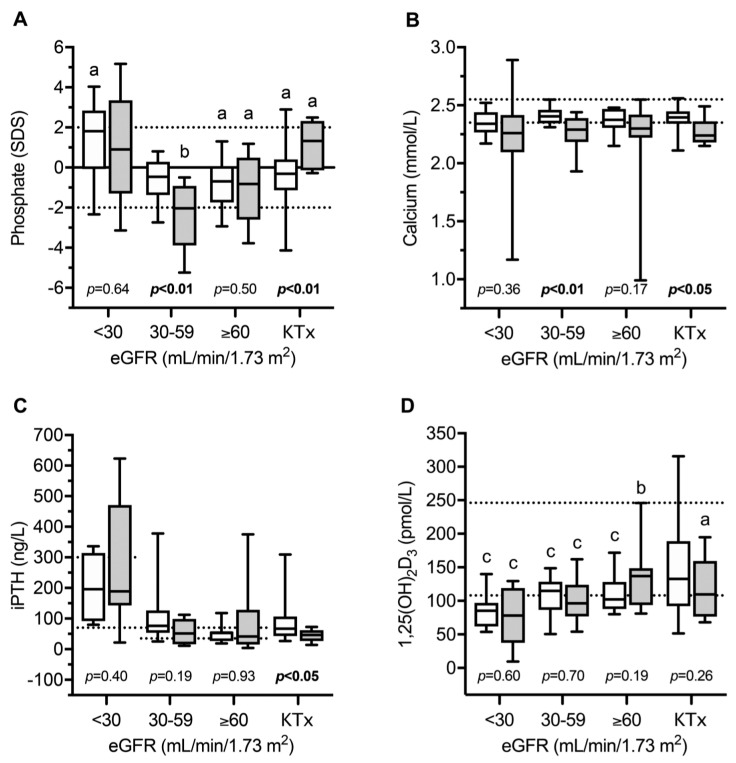
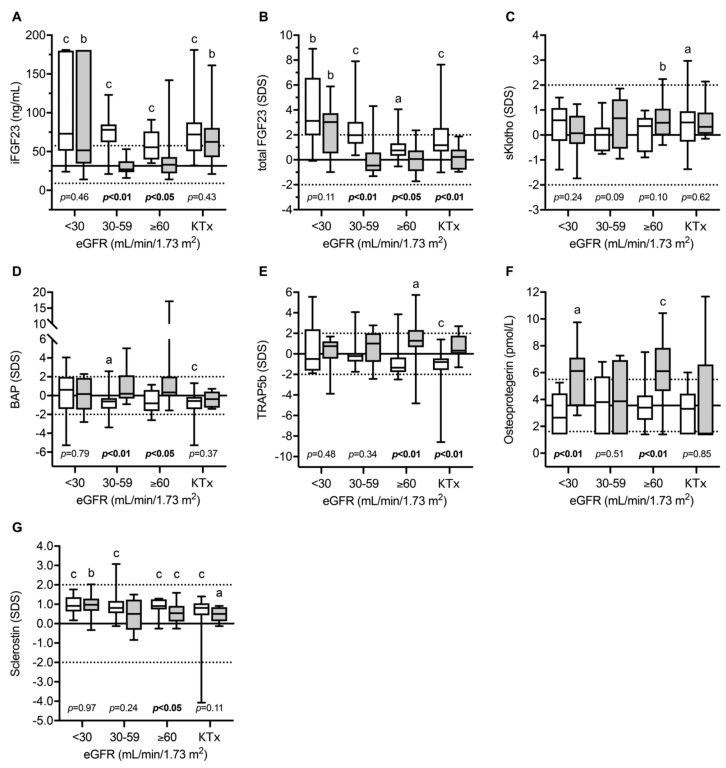
Cystinosis Metabolic Bone Disease (CMBD) has emerged during the last decade as a well-recognized, long-term complication in patients suffering from infantile nephropathic cystinosis (INC), resulting in significant morbidity and impaired quality of life in teenagers and adults with INC. Its underlying pathophysiology is complex and multifactorial, associating complementary, albeit distinct entities, in addition to ordinary mineral and bone disorders observed in other types of chronic kidney disease. Amongst these long-term consequences are renal Fanconi syndrome, hypophosphatemic rickets, malnutrition, hormonal abnormalities, muscular impairment, and intrinsic cellular bone defects in bone cells, due to CTNS mutations. Recent research data in the field have demonstrated abnormal mineral regulation, intrinsic bone defects, cysteamine toxicity, muscle wasting and, likely interleukin-1-driven inflammation in the setting of CMBD. Here we summarize these new pathophysiological deregulations and discuss the crucial interplay between bone and muscle in INC. In future, vitamin D and/or biotherapies targeting the IL1β pathway may improve muscle wasting and subsequently CMBD, but this remains to be proven.
Keywords: bone-muscle wasting; cysteamine; fibroblast growth factor 23; fractures; infantile nephropathic cystinosis; leptin; osteoclasts; sclerostin.
Conflict of interest statement
D.H. received speaker fees and research grants from Horizon and Chiesi. The other authors declare no conflict of interest.
Figures
Similar articles
-
Bone Disease in Nephropathic Cystinosis: Beyond Renal Osteodystrophy.Int J Mol Sci. 2020 Apr 28;21(9):3109. doi: 10.3390/ijms21093109. Int J Mol Sci. 2020. PMID: 32354056 Free PMC article. Review.
-
Vitamin D repletion ameliorates adipose tissue browning and muscle wasting in infantile nephropathic cystinosis-associated cachexia.J Cachexia Sarcopenia Muscle. 2020 Feb;11(1):120-134. doi: 10.1002/jcsm.12497. Epub 2019 Nov 13. J Cachexia Sarcopenia Muscle. 2020. PMID: 31721480 Free PMC article.
-
Targeting interleukin-1 for reversing fat browning and muscle wasting in infantile nephropathic cystinosis.J Cachexia Sarcopenia Muscle. 2021 Oct;12(5):1296-1311. doi: 10.1002/jcsm.12744. Epub 2021 Jun 30. J Cachexia Sarcopenia Muscle. 2021. PMID: 34196133 Free PMC article.
-
Management of bone disease in cystinosis: Statement from an international conference.J Inherit Metab Dis. 2019 Sep;42(5):1019-1029. doi: 10.1002/jimd.12134. Epub 2019 Aug 5. J Inherit Metab Dis. 2019. PMID: 31177550 Free PMC article.
-
Skeletal implications and management of cystinosis: three case reports and literature review.Bonekey Rep. 2016 Aug 17;5:828. doi: 10.1038/bonekey.2016.55. eCollection 2016. Bonekey Rep. 2016. PMID: 27579165 Free PMC article. Review.
Cited by
-
Morphological changes and their associations with clinical parameters in children with nephropathic cystinosis and chronic kidney disease prior to kidney replacement therapy over 25 years.Pediatr Nephrol. 2024 Oct;39(10):3067-3077. doi: 10.1007/s00467-024-06421-6. Epub 2024 Jun 8. Pediatr Nephrol. 2024. PMID: 38850407 Free PMC article.
-
Chest configuration in children and adolescents with infantile nephropathic cystinosis compared with other chronic kidney disease entities and its clinical determinants.Pediatr Nephrol. 2023 Dec;38(12):3989-3999. doi: 10.1007/s00467-023-06058-x. Epub 2023 Jul 7. Pediatr Nephrol. 2023. PMID: 37415042 Free PMC article.
-
Addressing the psychosocial aspects of transition to adult care in patients with cystinosis.Pediatr Nephrol. 2024 Oct;39(10):2861-2874. doi: 10.1007/s00467-024-06345-1. Epub 2024 Mar 22. Pediatr Nephrol. 2024. PMID: 38517536 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
