

Non-invasive intradermal imaging of cystine crystals in cystinosis
- PMID: 33661986
- PMCID: PMC7932553
- DOI: 10.1371/journal.pone.0247846
Non-invasive intradermal imaging of cystine crystals in cystinosis
Abstract
Importance: Development of noninvasive methodology to reproducibly measure tissue cystine crystal load to assess disease status and guide clinical care in cystinosis, an inherited lysosomal storage disorder characterized by widespread cystine crystal accumulation.
Objective: To develop an unbiased and semi-automated imaging methodology to quantify dermal cystine crystal accumulation in patients to correlate with disease status.
Design, setting and participants: 101 participants, 70 patients and 31 healthy controls, were enrolled at the University of California, San Diego, Cystinosis Clinics, Rady Children's Hospital, San Diego and at the annual Cystinosis Research Foundation family conference for an ongoing prospective longitudinal cohort study of cystinosis patients with potential yearly follow-up.
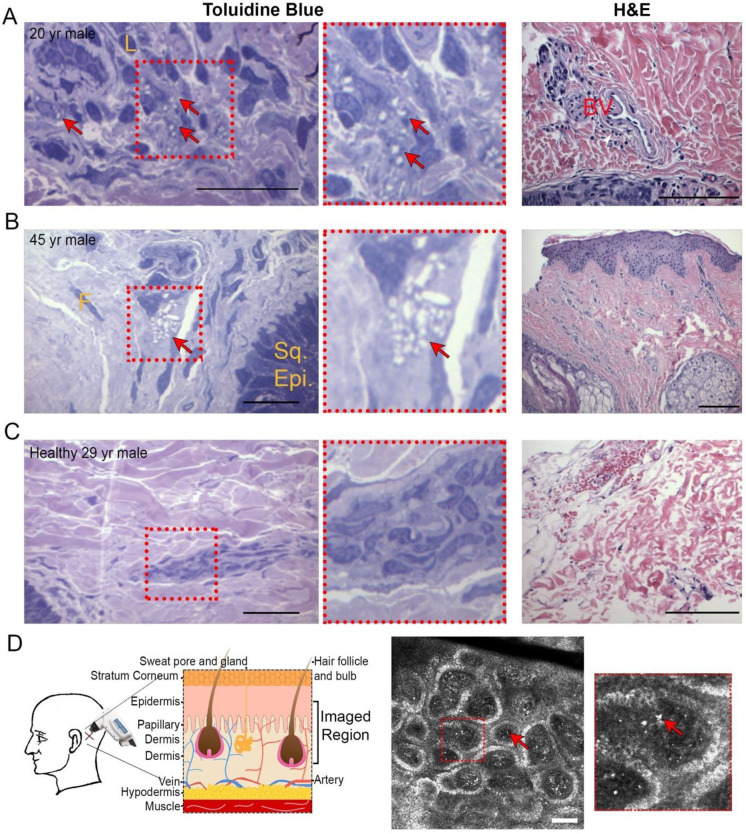
Exposures: Intradermal reflectance confocal microscopy (RCM) imaging, blood collection via standard venipuncture, medical record collection, and occasional skin punch biopsies.
Main outcomes and measures: The primary outcome was to establish an automated measure of normalized confocal crystal volume (nCCV) for each subject. Secondary analysis examined the association of nCCV with various clinical indicators to assess nCCV's possible predictive potential.
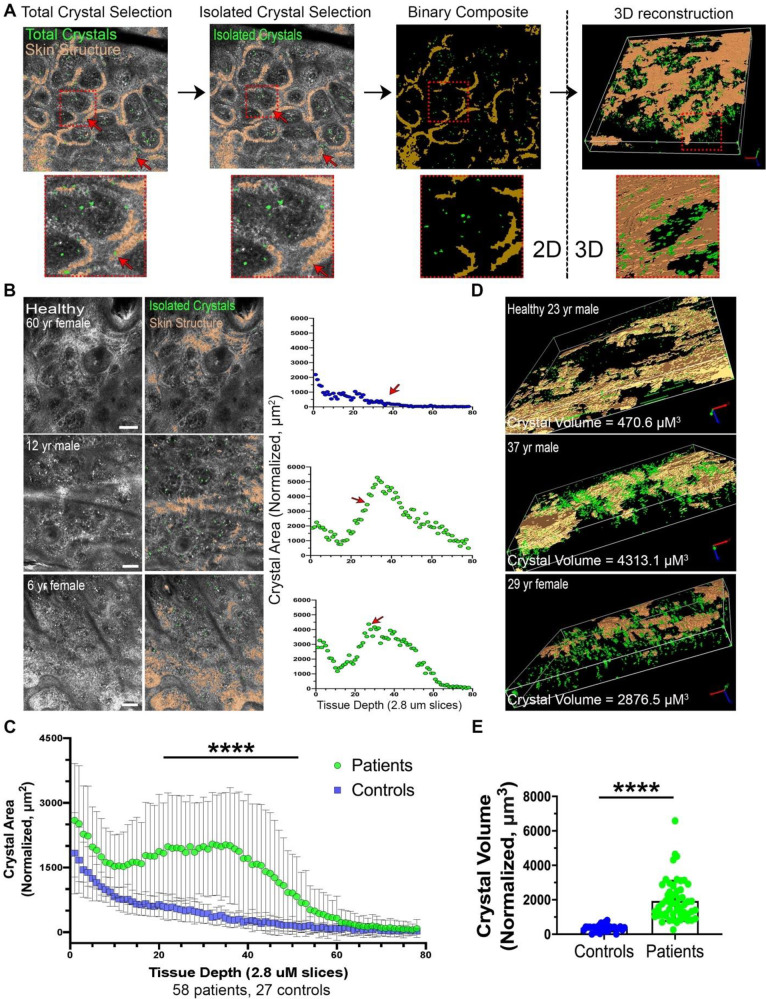
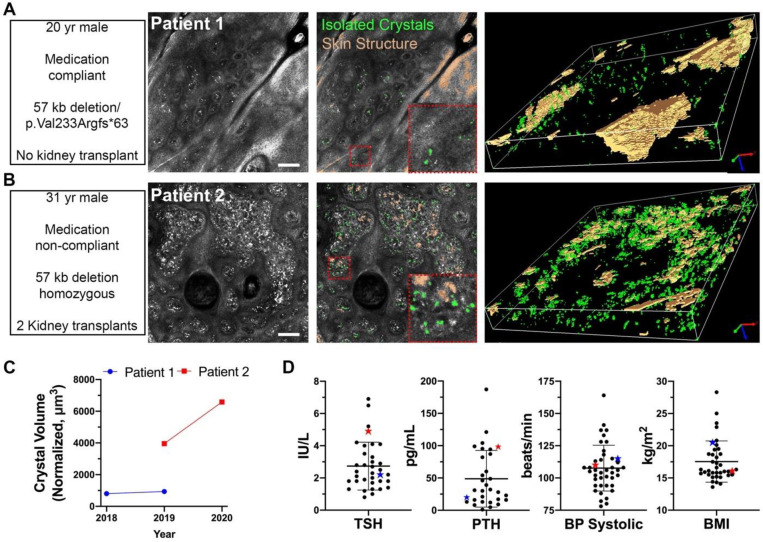
Results: Over 2 years, 57 patients diagnosed with cystinosis (median [range] age: 15.1 yrs [0.8, 54]; 41.4% female) were intradermally assessed by RCM to produce 84 image stacks. 27 healthy individuals (38.7 yrs [10, 85]; 53.1% female) were also imaged providing 37 control image stacks. Automated 2D crystal area quantification revealed that patients had significantly elevated crystal accumulation within the superficial dermis. 3D volumetric analysis of this region was significantly higher in patients compared to healthy controls (mean [SD]: 1934.0 μm3 [1169.1] for patients vs. 363.1 μm3 [194.3] for controls, P<0.001). Medical outcome data was collected from 43 patients with infantile cystinosis (media [range] age: 11 yrs [0.8, 54]; 51% female). nCCV was positively associated with hypothyroidism (OR = 19.68, 95% CI: [1.60, 242.46], P = 0.02) and stage of chronic kidney disease (slope estimate = 0.53, 95%CI: [0.05, 1.00], P = 0.03).
Conclusions and relevance: This study used non-invasive RCM imaging to develop an intradermal cystine crystal quantification method. Results showed that cystinosis patients had increased nCCV compared to healthy controls. Level of patient nCCV correlated with several clinical outcomes suggesting nCCV may be used as a potential new biomarker for cystinosis to monitor long-term disease control and medication compliance.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: Stephanie Cherqui is inventor on a patent entitled “Methods of treating mitochondrial disorders” (#20378-201301) and co-inventor on a patent entitled “Methods of treating lysosomal disorders” (#20378-202488). She is a cofounder, shareholder and a member of both the Scientific Board and Board of Directors of Stelios Therapeutics Inc. Stephanie Cherqui also serves as a member of the Scientific Review Board and Board of Trustees of the Cystinosis Research Foundation. The terms of this arrangement have been reviewed and approved by the University of California San Diego in accordance with its conflict of interest policies. This does not alter our adherence to PLOS ONE policies on sharing data and materials. There are no other patents, products in development or marketed products associated with this research to declare.
Figures
Similar articles
-
In vivo reflectance confocal microscopy of the skin: a noninvasive means of assessing body cystine accumulation in infantile cystinosis.J Am Acad Dermatol. 2013 Apr;68(4):e111-e116. doi: 10.1016/j.jaad.2011.08.010. Epub 2011 Oct 2. J Am Acad Dermatol. 2013. PMID: 21963264
-
Spectral domain optical coherence tomography-based retinochoroidal cystine crystal score: a window into infantile nephropathic cystinosis.Br J Ophthalmol. 2023 Feb;107(2):234-241. doi: 10.1136/bjophthalmol-2021-319612. Epub 2021 Sep 16. Br J Ophthalmol. 2023. PMID: 34531199 Free PMC article.
-
Examination of corneal deposits in nephropathic cystinosis using in vivo confocal microscopy and anterior segment optical coherence tomography: an age-dependent cross sectional study.BMC Ophthalmol. 2020 Feb 26;20(1):73. doi: 10.1186/s12886-020-01336-w. BMC Ophthalmol. 2020. PMID: 32102651 Free PMC article.
-
Corneal crystals in nephropathic cystinosis: natural history and treatment with cysteamine eyedrops.Mol Genet Metab. 2000 Sep-Oct;71(1-2):100-20. doi: 10.1006/mgme.2000.3062. Mol Genet Metab. 2000. PMID: 11001803 Review.
-
NIH conference. Cystinosis: progress in a prototypic disease.Ann Intern Med. 1988 Oct 1;109(7):557-69. doi: 10.7326/0003-4819-109-7-557. Ann Intern Med. 1988. PMID: 3048161 Review.
Cited by
-
Biomarkers in Nephropathic Cystinosis: Current and Future Perspectives.Cells. 2022 Jun 4;11(11):1839. doi: 10.3390/cells11111839. Cells. 2022. PMID: 35681534 Free PMC article. Review.
-
Hematopoietic Stem Cell Gene Therapy for Cystinosis: From Bench-to-Bedside.Cells. 2021 Nov 23;10(12):3273. doi: 10.3390/cells10123273. Cells. 2021. PMID: 34943781 Free PMC article. Review.
References
-
- Ivanova E, De Leo MG, De Matteis MA, Levtchenko E. Cystinosis: clinical presentation, pathogenesis and treatment. Pediatric endocrinology reviews: PER. 2014;12 Suppl 1:176–84. . - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
