

Identification and characterisation of the high-risk surgical population in the United Kingdom
- PMID: 16749940
- PMCID: PMC1550954
- DOI: 10.1186/cc4928
Identification and characterisation of the high-risk surgical population in the United Kingdom
Abstract
Introduction: Little is known about mortality rates following general surgical procedures in the United Kingdom. Deaths are most common in the 'high-risk' surgical population consisting mainly of older patients, with coexisting medical disease, who undergo major surgery. Only limited data are presently available to describe this population. The aim of the present study was to estimate the size of the high-risk general surgical population and to describe the outcome and intensive care unit (ICU) resource use.
Methods: Data on inpatient general surgical procedures and ICU admissions in 94 National Health Service hospitals between January 1999 and October 2004 were extracted from the Intensive Care National Audit & Research Centre database and the CHKS database. High-risk surgical procedures were defined prospectively as those for which the mortality rate was 5% or greater.
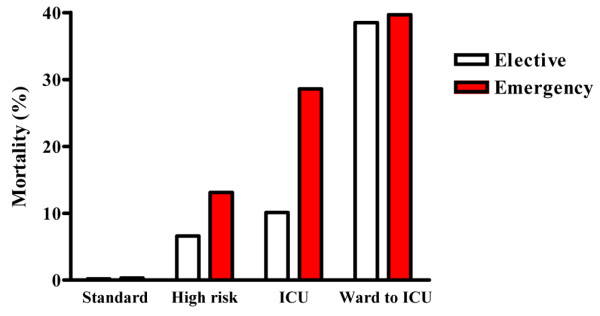
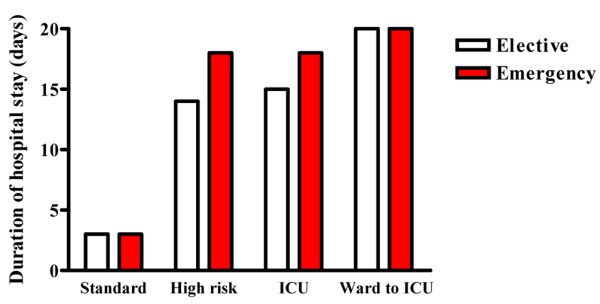
Results: There were 4,117,727 surgical procedures; 2,893,432 were elective (12,704 deaths; 0.44%) and 1,224,295 were emergencies (65,674 deaths; 5.4%). A high-risk population of 513,924 patients was identified (63,340 deaths; 12.3%), which accounted for 83.8% of deaths but for only 12.5% of procedures. This population had a prolonged hospital stay (median, 16 days; interquartile range, 9-29 days). There were 59,424 ICU admissions (11,398 deaths; 19%). Among admissions directly to the ICU following surgery, there were 31,633 elective admissions with 3,199 deaths (10.1%) and 24,764 emergency admissions with 7,084 deaths (28.6%). The ICU stays were short (median, 1.6 days; interquartile range, 0.8-3.7 days) but hospital admissions for those admitted to the ICU were prolonged (median, 16 days; interquartile range, 10-30 days). Among the ICU population, 40.8% of deaths occurred after the initial discharge from the ICU. The highest mortality rate (39%) occurred in the population admitted to the ICU following initial postoperative care on a standard ward.
Conclusion: A large high-risk surgical population accounts for 12.5% of surgical procedures but for more than 80% of deaths. Despite high mortality rates, fewer than 15% of these patients are admitted to the ICU.
Figures
Similar articles
-
Long-term mortality outcome associated with prolonged admission to the ICU.Chest. 2006 Apr;129(4):954-9. doi: 10.1378/chest.129.4.954. Chest. 2006. PMID: 16608944
-
Community-acquired pneumonia on the intensive care unit: secondary analysis of 17,869 cases in the ICNARC Case Mix Programme Database.Crit Care. 2006;10 Suppl 2(Suppl 2):S1. doi: 10.1186/cc4927. Crit Care. 2006. PMID: 16934135 Free PMC article.
-
Is postoperative intensive care unit admission a prerequisite for elective craniotomy?J Neurosurg. 2011 Dec;115(6):1236-41. doi: 10.3171/2011.8.JNS11105. Epub 2011 Sep 2. J Neurosurg. 2011. PMID: 21888476
-
ICU admission after surgery: who benefits?Curr Opin Crit Care. 2017 Oct;23(5):424-429. doi: 10.1097/MCC.0000000000000448. Curr Opin Crit Care. 2017. PMID: 28777159 Review.
-
Intensive care utilisation after elective surgery in Australia and New Zealand: getting the balance right.Aust Health Rev. 2023 Dec;47(6):718-720. doi: 10.1071/AH23187. Aust Health Rev. 2023. PMID: 38011832 Review.
Cited by
-
The Use of Pressure Recording Analytical Method in Patients Undergoing Endovascular Repair for Abdominal Aortic Aneurysm: The Impact on Clinical Decisions for the Appropriate Postoperative Setting and Cost-effective Analysis.Acta Med Acad. 2024 Apr;53(1):10-23. doi: 10.5644/ama2006-124.442. Acta Med Acad. 2024. PMID: 38984696 Free PMC article.
-
Stroke volume variation to guide fluid therapy: is it suitable for high-risk surgical patients? A terminated randomized controlled trial.Perioper Med (Lond). 2015 Jul 22;4:6. doi: 10.1186/s13741-015-0016-x. eCollection 2015. Perioper Med (Lond). 2015. PMID: 26203353 Free PMC article.
-
Asymmetric dimethylarginine predicts perioperative cardiovascular complications in patients undergoing medium-to-high risk non-cardiac surgery.J Int Med Res. 2020 Aug;48(8):300060520940450. doi: 10.1177/0300060520940450. J Int Med Res. 2020. PMID: 32842812 Free PMC article. Clinical Trial.
-
Clinical review: Goal-directed therapy-what is the evidence in surgical patients? The effect on different risk groups.Crit Care. 2013 Mar 5;17(2):209. doi: 10.1186/cc11823. Crit Care. 2013. PMID: 23672779 Free PMC article.
-
Current practice in hemodynamic monitoring and management in high-risk surgery patients: a national survey of Korean anesthesiologists.Korean J Anesthesiol. 2013 Jul;65(1):19-32. doi: 10.4097/kjae.2013.65.1.19. Epub 2013 Jul 19. Korean J Anesthesiol. 2013. PMID: 23904935 Free PMC article.
References
-
- Campling EA, Devlin HB, Lunn JN. Report of the National Confidential Enquiry into Peri-Operative Deaths. London: NCEPOD; 1990.
-
- Cullinane M, Gray AJ, Hargraves CM, Lansdown M, Martin IC, Schubert M. The 2003 Report of the National Confidential Enquiry into Peri-Operative Deaths. London: NCEPOD; 2003.
-
- Quality and Performance in the NHS: NHS Performance Indicators. London: NHS Executive; 2000.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
